Table of Contents
Introduction
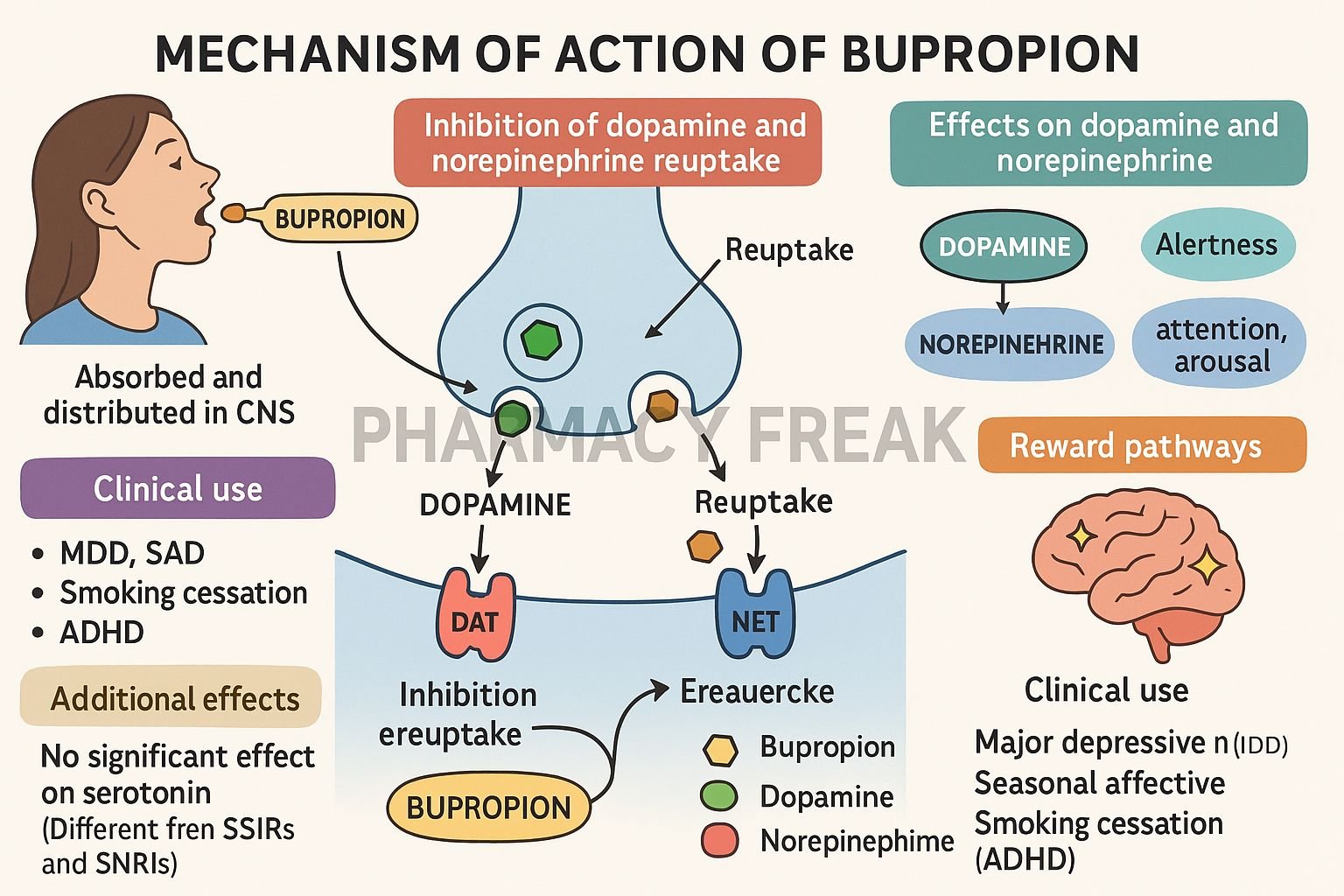
Bupropion is an atypical antidepressant primarily used to treat major depressive disorder, seasonal affective disorder, and as an aid for smoking cessation. Unlike SSRIs, bupropion exerts its effects via modulation of dopamine and norepinephrine neurotransmission, offering a unique mechanism without significant serotonergic side effects.
Step-by-Step Mechanism of Action
- Inhibition of norepinephrine reuptake
Bupropion inhibits the norepinephrine transporter (NET), increasing extracellular norepinephrine in synapses. - Inhibition of dopamine reuptake
It also inhibits the dopamine transporter (DAT), elevating dopamine levels, especially in brain areas related to mood and motivation. - No direct effect on serotonin
Bupropion has no significant serotonin reuptake inhibition, reducing the risk of sexual dysfunction, weight gain, and emotional blunting. - Nicotine receptor antagonism
Bupropion acts as a non-competitive antagonist of nicotinic acetylcholine receptors, aiding in smoking cessation by reducing cravings and withdrawal. - Indirect downstream effects
Elevated norepinephrine and dopamine increase brain-derived neurotrophic factor (BDNF) and neuronal resilience, supporting antidepressant activity.

Pharmacokinetic Parameters
| Parameter | Value |
|---|---|
| Route | Oral (tablets, sustained-release) |
| Bioavailability | ~5–20% |
| Time to peak (Tmax) | ~2 hours (immediate release); ~5 hours (SR/XL) |
| Protein Binding | ~84% |
| Metabolism | Hepatic CYP2B6 → active metabolites (hydroxy-, erythro-, threohydrobupropion) |
| Half-life | ~21 hours (parent); metabolites ~20–37 hours |
| Excretion | Renal (~87%); fecal (~10%) |
Clinical Uses
- Major depressive disorder
- Seasonal affective disorder
- Smoking cessation aid (as Zyban)
- Off-label uses: ADHD, neuropathic pain, weight management adjunct
Adverse Effects
- Stimulant-like effects: insomnia, dry mouth, headache
- Tachycardia, elevated blood pressure in some patients
- Seizure risk, especially at doses >450 mg/day or in susceptible individuals
- GI upset, diaphoresis, tremor
- Low risk: sexual dysfunction, weight gain, sedation
Comparative Analysis
| Drug | NE & DA Reuptake | Serotonin Effect | Seizure Risk | Uses |
|---|---|---|---|---|
| Bupropion | Moderate | None | Moderate–High | Depression, cessation |
| SSRIs (e.g. fluoxetine) | None to low | High | Low | Depression, anxiety |
| Venlafaxine | High (NE), moderate (5-HT) | Moderate | Moderate | Severe depression, pain |
MCQs (15)
- Bupropion primarily inhibits reuptake of which neurotransmitters?
a) Serotonin & GABA b) Dopamine & norepinephrine c) Glutamate & acetylcholine d) Histamine & serotonin
Answer: b) Dopamine & norepinephrine - It lacks significant inhibition of which transporter?
a) DAT b) NET c) SERT d) VMAT
Answer: c) SERT - Bupropion assists smoking cessation by antagonizing:
a) Nicotinic receptors b) Muscarinic receptors c) Adrenergic receptors d) Dopaminergic receptors
Answer: a) Nicotinic receptors - A key advantage over SSRIs is:
a) Higher sexual dysfunction risk b) Weight gain c) Lower risk of sexual side effects d) Strong sedative effect
Answer: c) Lower risk of sexual side effects - Which adverse effect is most concerning at high doses?
a) Seizure b) Weight gain c) Hypotension d) Sedation
Answer: a) Seizure - Major metabolites are produced via which enzyme?
a) CYP3A4 b) CYP2B6 c) CYP2D6 d) CYP1A2
Answer: b) CYP2B6 - Bupropion has a half-life of approximately:
a) 5 hours b) 21 hours c) 48 hours d) 72 hours
Answer: b) 21 hours - Which off-label use is common?
a) Hypertension b) ADHD c) Asthma d) Depression
Answer: b) ADHD - Bupropion is contraindicated in patients with:
a) Hypothyroidism b) Epilepsy c) Diabetes d) Glaucoma
Answer: b) Epilepsy - Compared to bupropion, SSRIs are more likely to cause:
a) Appetite increase b) Seizures c) Stimulant effects d) Insomnia
Answer: a) Appetite increase - Protein binding is approximately:
a) 30% b) 60% c) 84% d) 100%
Answer: c) 84% - Time to peak for SR formulation is about:
a) 1 hour b) 3 hours c) 5 hours d) 10 hours
Answer: c) 5 hours - One key stimulant-like adverse effect is:
a) Sedation b) Dry mouth c) Bradycardia d) Diarrhea
Answer: b) Dry mouth - Its use in neuropathic pain is due to:
a) Histamine blockade b) NE elevation c) Serotonin reuptake d) Opioid agonism
Answer: b) NE elevation - Recommended maximum daily dose to minimize seizure risk:
a) 150 mg b) 300 mg c) 450 mg d) 600 mg
Answer: c) 450 mg
FAQs
1. Does bupropion cause sexual dysfunction?
No—bupropion rarely causes sexual side effects, making it useful when these are a concern.
2. When should doses exceed 450 mg/day?
They generally should not—higher doses significantly increase seizure risk.
3. How quickly does it improve depressive symptoms?
Typically within 4–6 weeks of treatment initiation.
4. Can it be used with nicotine patches?
Yes—can enhance smoking cessation outcomes but monitor for combined side effects.
5. Is it safe in adolescents?
It is approved for adults; use in adolescents requires caution regarding seizure risk.
References
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics, 13th Edition
- KD Tripathi. Essentials of Medical Pharmacology, 8th Edition
- DrugBank: Bupropion pharmacology summary
- StatPearls: Pharmacology of bupropion and smoking cessation
- PubMed review: Dopamine–norepinephrine mechanisms in depression and cessation

