
Table of Contents
Introduction
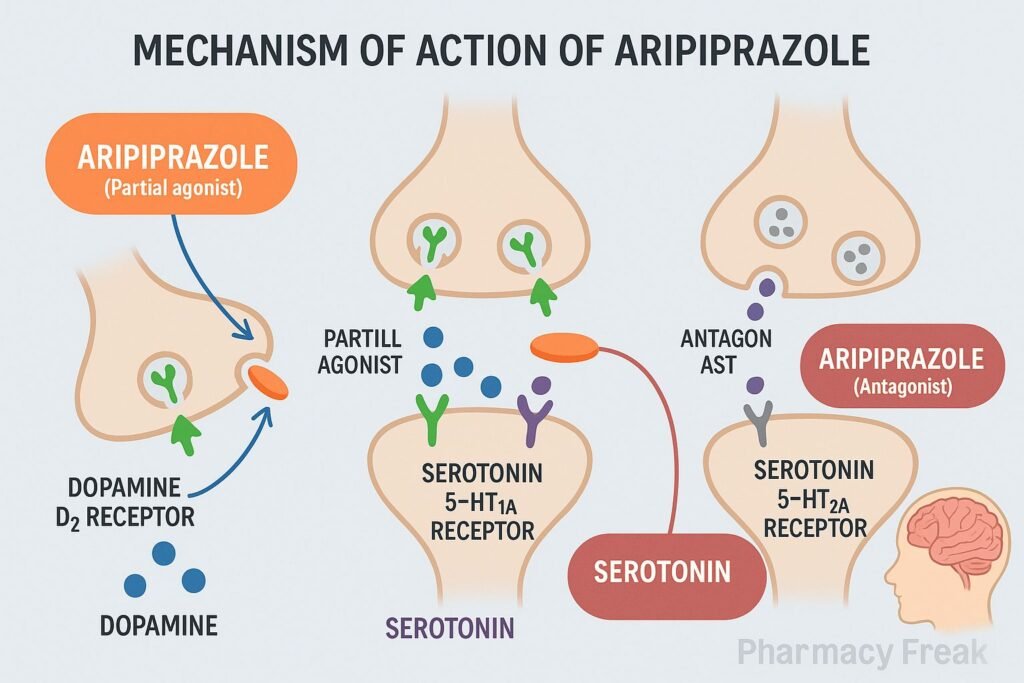
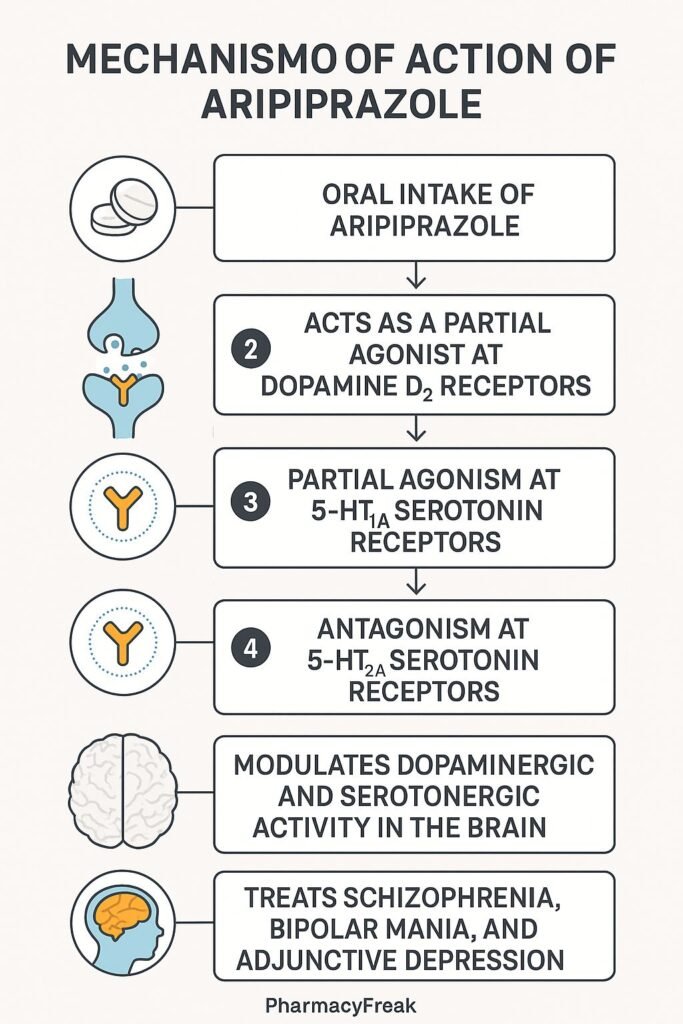
Aripiprazole is a third-generation atypical antipsychotic approved for treating schizophrenia, bipolar disorder, depression (as an adjunct), Tourette’s syndrome, and irritability in autism. It is pharmacologically unique for its role as a partial agonist at dopamine D₂ and serotonin 5‑HT₁A receptors, and as an antagonist at serotonin 5‑HT₂A receptors, allowing it to modulate neurotransmission rather than fully block it.
Step-by-Step Mechanism of Action
- Partial Agonist at Dopamine D₂ Receptors
Aripiprazole partially activates D₂ receptors, reducing excessive dopamine signaling in mesolimbic pathways (psychosis) and enhancing it in mesocortical pathways (cognition and mood). - Partial Agonist at 5‑HT₁A Receptors
This contributes to mood regulation and may reduce anxiety and depressive symptoms. - Antagonist at 5‑HT₂A Receptors
Blocking this receptor helps minimize extrapyramidal symptoms and supports antipsychotic effects. - Functional Selectivity
Aripiprazole behaves differently depending on receptor density and dopamine tone in different brain regions, enabling a “dopamine stabilizer” profile.
Pharmacokinetic Parameters
| Parameter | Value |
|---|---|
| Bioavailability | 87–90% (oral) |
| Protein Binding | >99% |
| Metabolism | Hepatic via CYP2D6 and CYP3A4 |
| Half-Life (Parent Drug) | ~75 hours |
| Half-Life (Metabolite) | ~94 hours |
| Excretion | 27% renal, 60% fecal |
Clinical Uses
- Schizophrenia (ages ≥13)
- Bipolar I disorder (mania and maintenance)
- Adjunct therapy in major depressive disorder
- Tourette’s syndrome
- Irritability associated with autism spectrum disorder
Adverse Effects
- Akathisia and restlessness
- Insomnia
- Mild weight gain
- Nausea, constipation
- Headache and dizziness
- Rare: tardive dyskinesia, neuroleptic malignant syndrome
- Low risk of extrapyramidal symptoms (EPS)
Comparative Analysis
| Feature | Aripiprazole | Risperidone / Haloperidol |
|---|---|---|
| D₂ Receptor Activity | Partial agonist | Full antagonist |
| 5‑HT₁A Activity | Partial agonist | Minimal or none |
| 5‑HT₂A Activity | Antagonist | Antagonist |
| EPS Risk | Low | Moderate to high |
| Dopamine Modulation | Region- and tone-sensitive | Blocks indiscriminately |
MCQs
1. What is aripiprazole’s action at D₂ receptors?
A. Full antagonist
B. Inverse agonist
C. Partial agonist
D. No effect
Answer: C
2. Aripiprazole acts as a partial agonist at which serotonin receptor?
A. 5‑HT₂A
B. 5‑HT₁A
C. 5‑HT₃
D. 5‑HT₄
Answer: B
3. Which serotonin receptor is blocked by aripiprazole?
A. 5‑HT₁A
B. 5‑HT₃
C. 5‑HT₂A
D. 5‑HT₆
Answer: C
4. Aripiprazole is primarily metabolized by:
A. CYP1A2
B. CYP2D6 and CYP3A4
C. CYP2C9
D. CYP2E1
Answer: B
5. What is the approximate half-life of aripiprazole?
A. 24 hours
B. 48 hours
C. 75 hours
D. 10 hours
Answer: C
6. The risk of extrapyramidal symptoms with aripiprazole is:
A. High
B. Moderate
C. Low
D. Unknown
Answer: C
7. Functional selectivity means aripiprazole:
A. Always activates receptors
B. Blocks all D₂ activity
C. Modulates effect based on brain region
D. Is a full agonist everywhere
Answer: C
8. Which of the following is NOT an approved use of aripiprazole?
A. Schizophrenia
B. Bipolar disorder
C. Tourette’s syndrome
D. Obsessive-compulsive disorder
Answer: D
9. Compared to typical antipsychotics, aripiprazole has:
A. Higher EPS risk
B. Lower efficacy
C. Lower EPS risk
D. Greater sedation
Answer: C
10. In dopamine-deficient areas, aripiprazole acts as a:
A. Strong antagonist
B. Partial agonist
C. Reuptake inhibitor
D. Full agonist
Answer: B
FAQs
1. Is aripiprazole a typical or atypical antipsychotic?
It is an atypical (third-generation) antipsychotic.
2. Why does it have fewer movement side effects?
Because it partially activates D₂ receptors rather than completely blocking them.
3. Can aripiprazole be used in depression?
Yes, it is approved as an adjunct treatment for major depressive disorder.
4. Does it need to be taken daily?
Yes, usually once daily due to its long half-life.
5. What makes aripiprazole unique?
Its partial agonism at dopamine and serotonin receptors allows it to stabilize rather than blunt neurotransmitter activity.
References
- DrugBank – Aripiprazole Mechanism & Receptor Activity
- NCBI PMC – Aripiprazole Pharmacologic Profile
- JAMA Psychiatry – Aripiprazole Review
- Goodman & Gilman’s: The Pharmacological Basis of Therapeutics


