
Table of Contents
Introduction
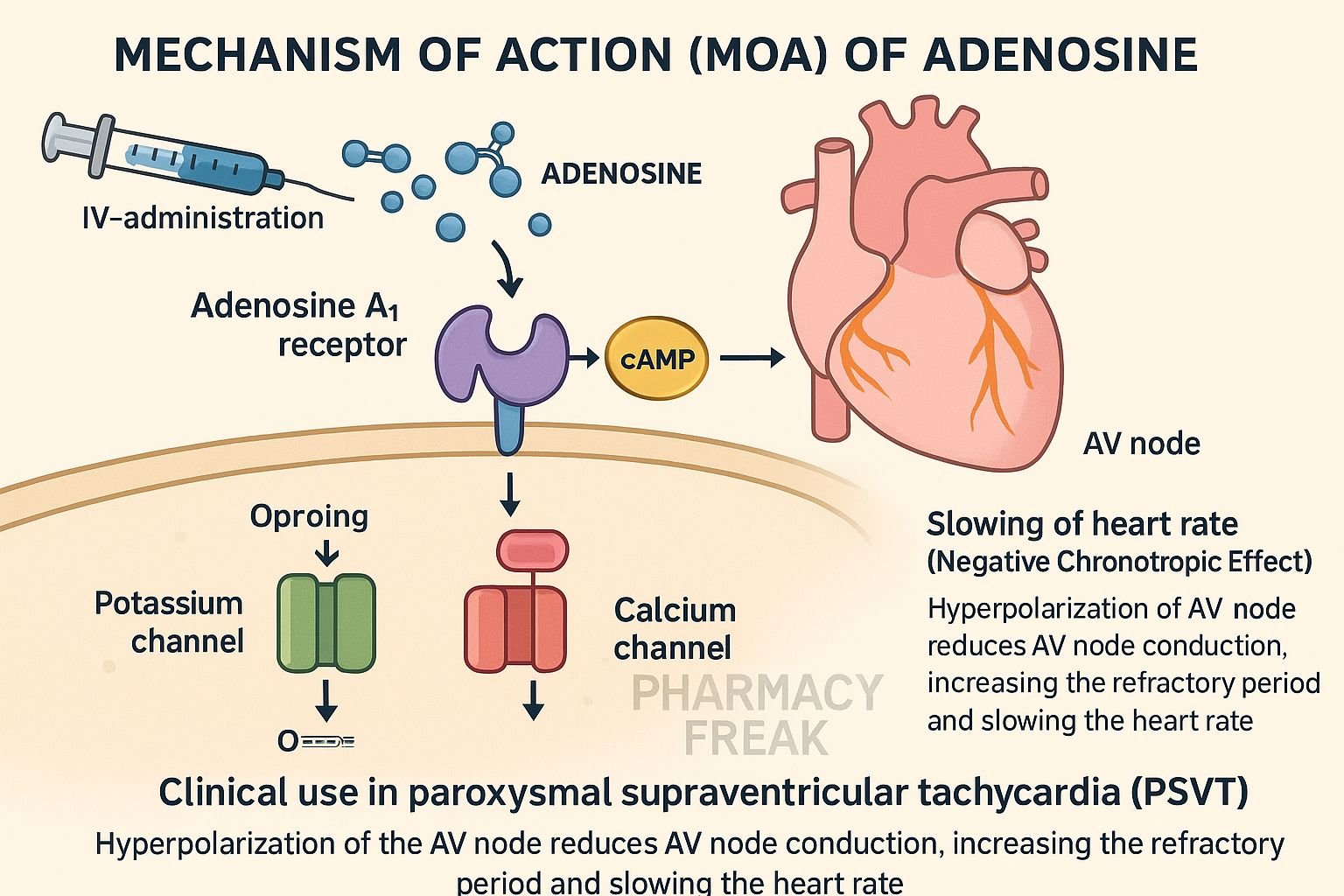
Adenosine is an endogenous purine nucleoside used intravenously for the acute termination of paroxysmal supraventricular tachycardia (PSVT). It acts on specific adenosine receptors in the heart to slow conduction through the atrioventricular (AV) node. Its ultra-short action and safety profile make it the treatment of choice for acute narrow-complex tachycardias.
Step-by-Step Mechanism of Action
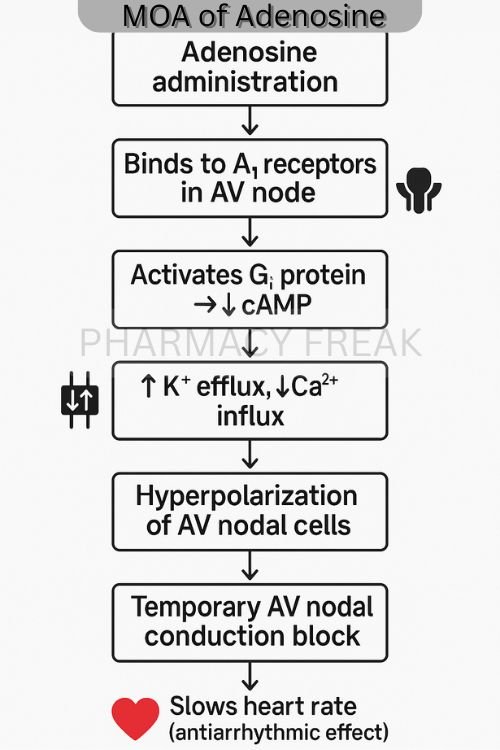
- Activation of A₁ receptors in the AV node
Adenosine binds to A₁ receptors (a subtype of Gᵢ-coupled receptors) on AV nodal tissue, resulting in decreased cyclic AMP (cAMP) levels. - Opening of potassium channels
The reduction in cAMP triggers the opening of inward-rectifier potassium channels (I_K,Ado), leading to efflux of K⁺ and hyperpolarization of AV nodal cells. - Suppression of AV nodal conduction and automaticity
Hyperpolarization prolongs AV nodal refractory periods and conduction time, effectively interrupting re-entrant tachycardia circuits. - Indirect reduction of calcium influx
Lower cAMP also reduces L-type calcium channel activity, further slowing impulse propagation through the AV node. - Ultra-short duration of action
Adenosine is rapidly metabolized by erythrocytes and vascular endothelial cells, resulting in a half-life of less than 10 seconds.
Pharmacokinetic Parameters
| Parameter | Value |
|---|---|
| Route of Administration | Intravenous (rapid bolus) |
| Distribution | Widespread; crosses cell membranes |
| Onset | 10–20 seconds |
| Half-life | <10 seconds |
| Metabolism | Uptake by red blood cells and vascular endothelium |
| Excretion | Metabolized endogenously; not excreted unchanged |
Clinical Uses
- Termination of paroxysmal supraventricular tachycardia (PSVT)
- Diagnostic agent to unmask atrial flutter or pre-excitation syndromes (e.g., WPW)
- Occasionally used in myocardial perfusion imaging studies
Adverse Effects
- Transient flushing, chest discomfort, dyspnea
- Lightheadedness, hypotension
- Bronchospasm in asthmatics
- Brief asystole or bradycardia
- Rare: AV block requiring intervention
Comparative Analysis
| Drug | Target Receptor | Onset | Half‑Life | Use in PSVT |
|---|---|---|---|---|
| Adenosine | A₁ receptor | 10–20 seconds | <10 seconds | First-line therapy |
| Verapamil | L-type Ca²⁺ channel blocker | Minutes | 30–60 minutes | Alternative |
| Diltiazem | L-type Ca²⁺ channel blocker | Minutes | 3–4 hours | Alternative |
MCQs (15 questions)
1. Adenosine terminates PSVT primarily by acting on which receptor?
a) β₁ b) A₂ c) A₁ d) M₂
Answer: c) A₁
2. The primary electrophysiologic change induced by adenosine is:
a) Sodium channel blockade
b) AV nodal hyperpolarization
c) Ventricular repolarization
d) Increased automaticity
Answer: b) AV nodal hyperpolarization
3. Adenosine works by reducing which intracellular messenger?
a) IP₃ b) DAG c) cGMP d) cAMP
Answer: d) cAMP
4. The typical onset time after IV bolus is:
a) Immediate b) 10–20 seconds c) 2 minutes d) 5 minutes
Answer: b) 10–20 seconds
5. Its half-life is approximately:
a) <10 seconds b) 1 minute c) 5 minutes d) 30 minutes
Answer: a) <10 seconds
6. A notable side effect in asthmatic patients is:
a) Diarrhea b) Bronchospasm c) Hypoglycemia d) Rash
Answer: b) Bronchospasm
7. Adenosine’s classification is:
a) Purine nucleoside b) Catecholamine c) Beta-blocker d) Calciums antagonist
Answer: a) Purine nucleoside
8. Which ion channel is activated by adenosine in AV node?
a) Sodium b) Calcium c) Inward-rectifier potassium d) Chloride
Answer: c) Inward-rectifier potassium
9. It is contraindicated in patients on:
a) Theophylline b) Nitrates c) ACE inhibitors d) Statins
Answer: a) Theophylline
10. Adenosine is ineffective in treating:
a) Atrial flutter b) AV nodal re-entrant tachycardia c) PSVT d) Wolf-Parkinson-White syndrome
Answer: a) Atrial flutter
11. Duration of AV block induced is:
a) Several minutes b) Brief (<20 seconds) c) Hours d) Prolonged days
Answer: b) Brief (<20 seconds)
12. Which statement is true?
a) It’s a long-term therapy b) Can worsen hypotension c) Slows AV conduction d) Increases contractility
Answer: c) Slows AV conduction
13. Drug is metabolized by:
a) Liver CYPs b) Renal excretion c) Red blood cells/endothelial uptake d) Plasma esterases
Answer: c) Red blood cells/endothelial uptake
14. First-line acute PSVT agent is:
a) Propranolol b) Adenosine c) Amiodarone d) Metoprolol
Answer: b) Adenosine
15. Administration route is:
a) Oral b) IV rapid push c) Subcutaneous d) Transdermal
Answer: b) IV rapid push
FAQs
1. Is adenosine effective for atrial flutter?
No—it may briefly slow conduction but won’t terminate the rhythm.
2. Can adenosine be repeated?
Yes, typically 6 mg–12 mg IV boluses may be repeated once if needed.
3. Should ECG monitoring accompany administration?
Absolutely—due to risk of transient AV block and bradycardia.
4. Is adenosine safe in pregnancy?
Yes, it’s considered safe for use during pregnancy for SVT.
5. What to expect after injection?
A brief pause in heartbeat (a few seconds), flushing or chest pressure, then return to normal rhythm.
References
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics, 13th Edition
- KD Tripathi. Essentials of Medical Pharmacology, 8th Edition
- StatPearls: Adenosine in cardiac arrhythmias
- PubMed: Pharmacodynamics of adenosine in PSVT
- PubMed: Adenosine receptor physiology
- StatPearls: Adenosine safety profile


