
Table of Contents
Introduction
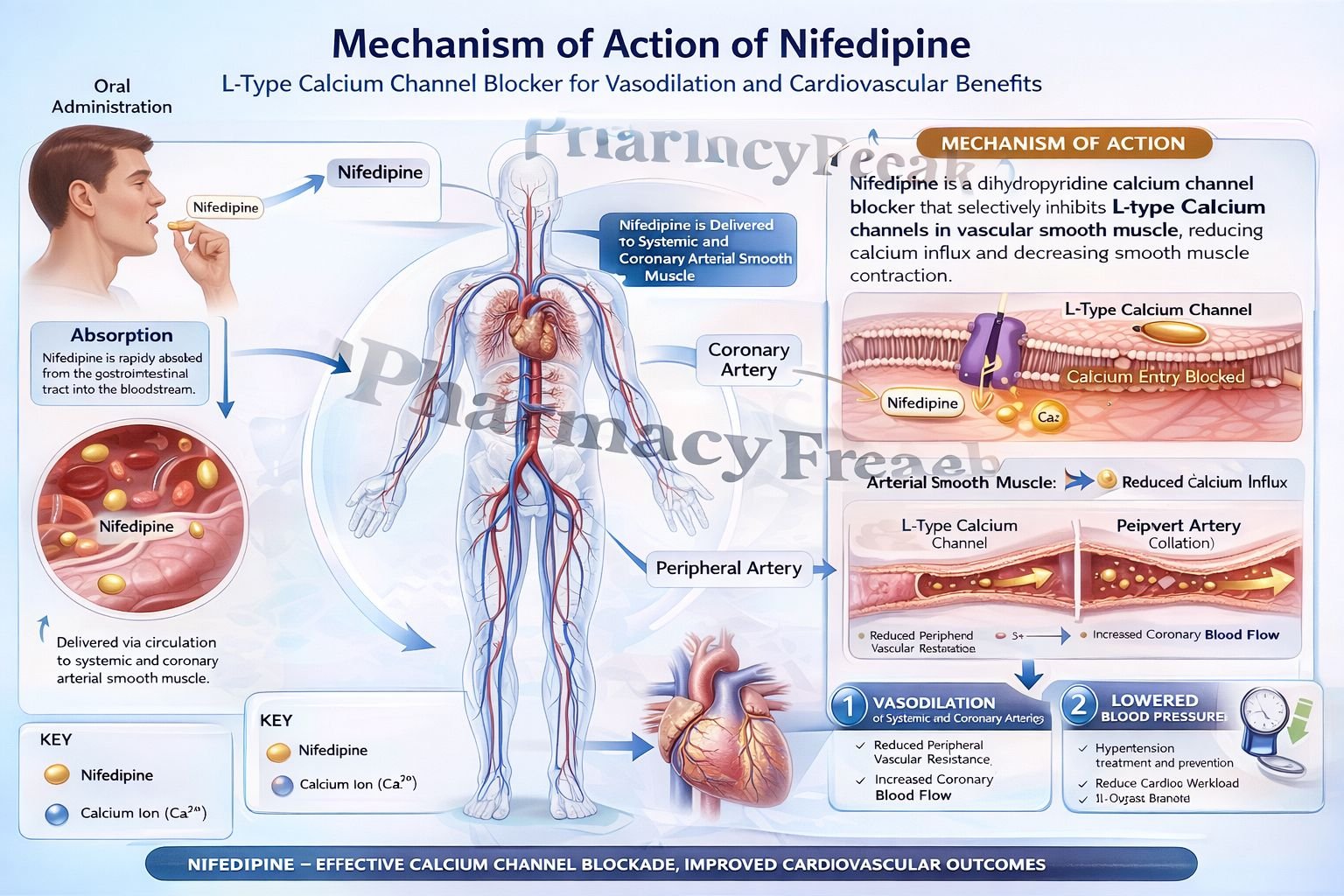
Nifedipine is a dihydropyridine calcium channel blocker widely used in the management of hypertension and angina. It primarily acts on vascular smooth muscle to produce vasodilation, thereby reducing blood pressure and improving coronary blood flow. Compared to non-dihydropyridines, nifedipine has a stronger effect on peripheral vasculature than on the heart.
Mechanism of Action (Step-wise)
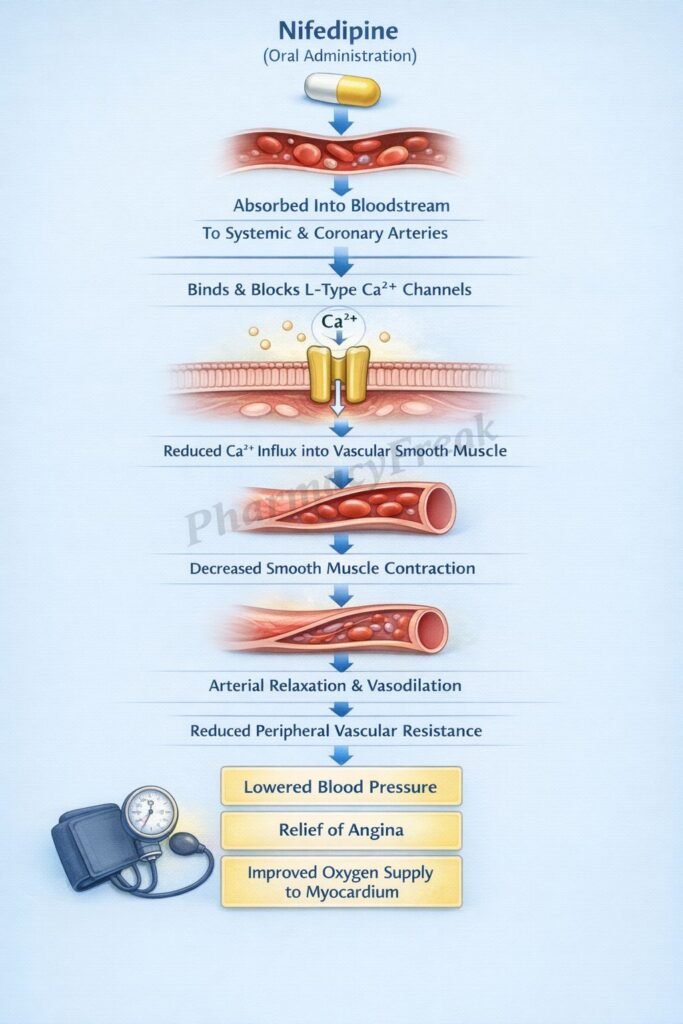
- Nifedipine selectively blocks L-type voltage-gated calcium channels.
- These channels are present in vascular smooth muscle and cardiac muscle.
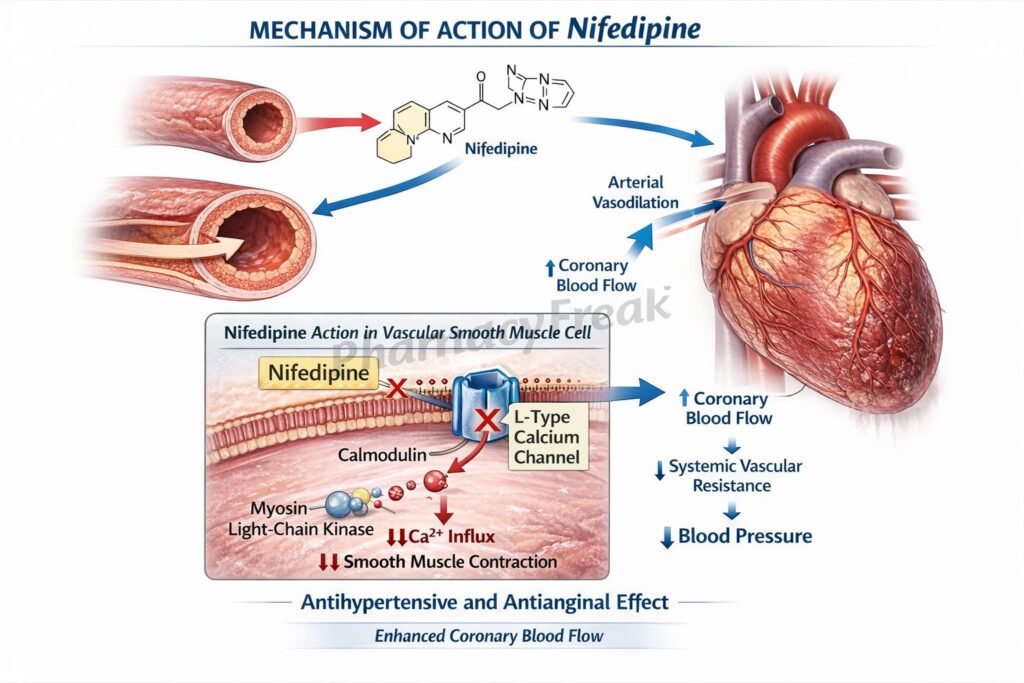
- Blockade reduces calcium influx into smooth muscle cells.
- Decreased intracellular calcium reduces activation of calmodulin.
- This leads to decreased activation of myosin light chain kinase (MLCK).
- Reduced MLCK activity decreases phosphorylation of myosin.
- This results in relaxation of vascular smooth muscle.
- Arteriolar vasodilation reduces systemic vascular resistance (afterload).
- Coronary vasodilation improves blood supply to the myocardium.
- The net effect is decreased blood pressure and improved oxygen delivery.
A key exam point is that nifedipine is a dihydropyridine calcium channel blocker that primarily causes vasodilation.
Pharmacokinetics
Nifedipine is administered orally and is well absorbed. It undergoes extensive first-pass metabolism in the liver, resulting in moderate bioavailability. It is highly protein-bound and metabolized mainly by CYP3A4 enzymes. It has a relatively short half-life, but extended-release formulations are available for once-daily dosing. It is excreted primarily via the kidneys.
Clinical Uses
Nifedipine is used in hypertension to lower blood pressure by reducing peripheral resistance. It is also used in angina pectoris to improve coronary blood flow and decrease myocardial oxygen demand. It is effective in vasospastic (Prinzmetal) angina due to its strong vasodilatory action. Additionally, it may be used in Raynaud phenomenon.
Adverse Effects
Common adverse effects include headache, flushing, dizziness, and peripheral edema due to vasodilation. Reflex tachycardia may occur as a compensatory response. Gingival hyperplasia is a known side effect. Hypotension may occur in excessive dosing.
Comparative Analysis
| Feature | Nifedipine | Verapamil | Diltiazem |
|---|---|---|---|
| Class | Dihydropyridine | Non-dihydropyridine | Non-dihydropyridine |
| Primary action | Vascular smooth muscle | Cardiac muscle | Cardiac + vascular |
| Effect on heart rate | Reflex increase | Decrease | Decrease |
| Vasodilation | Strong | Moderate | Moderate |
| Use | Hypertension, angina | Arrhythmias, angina | Hypertension, angina |
| AV conduction | Minimal effect | Strong inhibition | Moderate inhibition |
Nifedipine differs from verapamil and diltiazem by having a stronger effect on vascular smooth muscle and minimal direct cardiac depression. It is more likely to cause reflex tachycardia due to potent vasodilation.
MCQs
- Nifedipine belongs to which class?
a) Beta blockers
b) Calcium channel blockers
c) ACE inhibitors
d) Diuretics
Answer: b) Calcium channel blockers
- Nifedipine blocks which channels?
a) Sodium channels
b) Calcium channels
c) Potassium channels
d) Chloride channels
Answer: b) Calcium channels
- Nifedipine primarily acts on:
a) Cardiac muscle
b) Vascular smooth muscle
c) Liver
d) Kidney
Answer: b) Vascular smooth muscle
- Blocking calcium channels leads to:
a) Increased contraction
b) Decreased contraction
c) No change
d) Increased sodium
Answer: b) Decreased contraction
- Nifedipine reduces:
a) Preload
b) Afterload
c) Heart rate directly
d) Blood glucose
Answer: b) Afterload
- Nifedipine is used in:
a) Asthma
b) Hypertension
c) Diabetes
d) Anemia
Answer: b) Hypertension
- A common adverse effect is:
a) Bradycardia
b) Headache
c) Hypoglycemia
d) Hypercalcemia
Answer: b) Headache
- Nifedipine may cause:
a) Bradycardia
b) Reflex tachycardia
c) Hypotension only
d) Hyperglycemia
Answer: b) Reflex tachycardia
- Nifedipine is metabolized by:
a) CYP2D6
b) CYP3A4
c) CYP1A2
d) CYP2C9
Answer: b) CYP3A4
- Nifedipine is effective in:
a) Stable angina only
b) Vasospastic angina
c) Arrhythmias
d) Diabetes
Answer: b) Vasospastic angina
- Compared to verapamil, nifedipine has:
a) More cardiac effect
b) Less vascular effect
c) More vascular effect
d) Same effect
Answer: c) More vascular effect
- Nifedipine causes vasodilation by:
a) Increasing calcium
b) Blocking calcium entry
c) Increasing sodium
d) Blocking potassium
Answer: b) Blocking calcium entry
FAQs
What is the mechanism of action of nifedipine?
It blocks L-type calcium channels, causing vasodilation and reduced blood pressure.
Why does nifedipine cause reflex tachycardia?
Due to rapid vasodilation and decreased blood pressure triggering sympathetic activation.
What type of angina is nifedipine most effective in?
Vasospastic (Prinzmetal) angina.
Does nifedipine affect heart conduction?
Minimal effect compared to non-dihydropyridines.
What is a common side effect?
Headache and flushing.
How does nifedipine lower blood pressure?
By reducing systemic vascular resistance (afterload).
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics – Calcium Channel Blockers
https://accessmedicine.mhmedical.com/book.aspx?bookid=3191
Katzung: Basic and Clinical Pharmacology – Cardiovascular Drugs
https://accessmedicine.mhmedical.com/content.aspx?bookid=3382
Tripathi: Essentials of Medical Pharmacology – Antihypertensives
https://www.jaypeedigital.com
Harrison’s Principles of Internal Medicine – Hypertension and Angina
https://accessmedicine.mhmedical.com

