Table of Contents
Introduction
Morphine is a potent opioid analgesic derived from opium and widely used for the management of moderate to severe pain. It acts primarily on opioid receptors in the central nervous system to produce analgesia, sedation, and euphoria. Morphine is considered the prototype opioid and is commonly used in postoperative pain, cancer pain, and acute coronary syndromes.
Mechanism of Action (Step-wise)
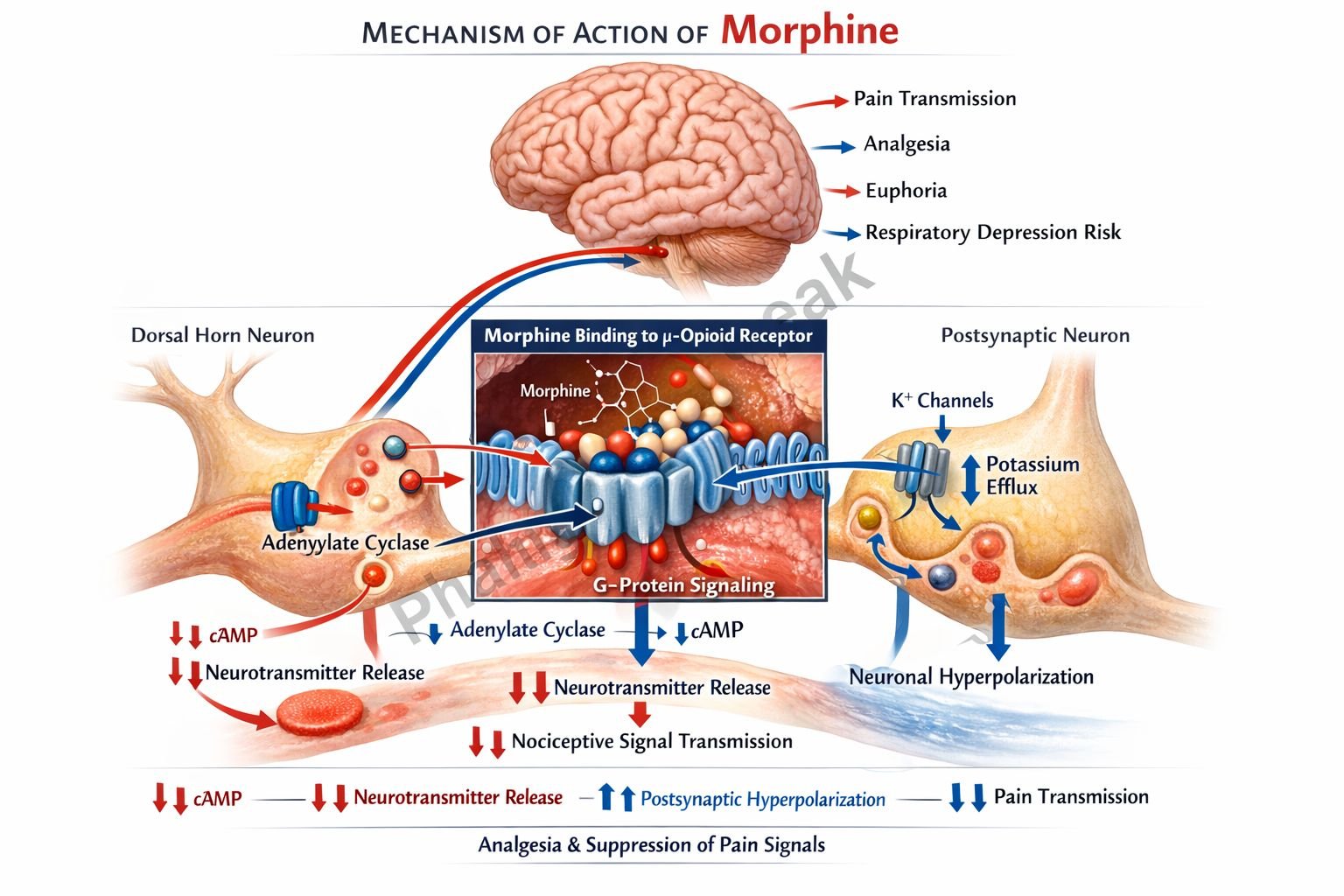
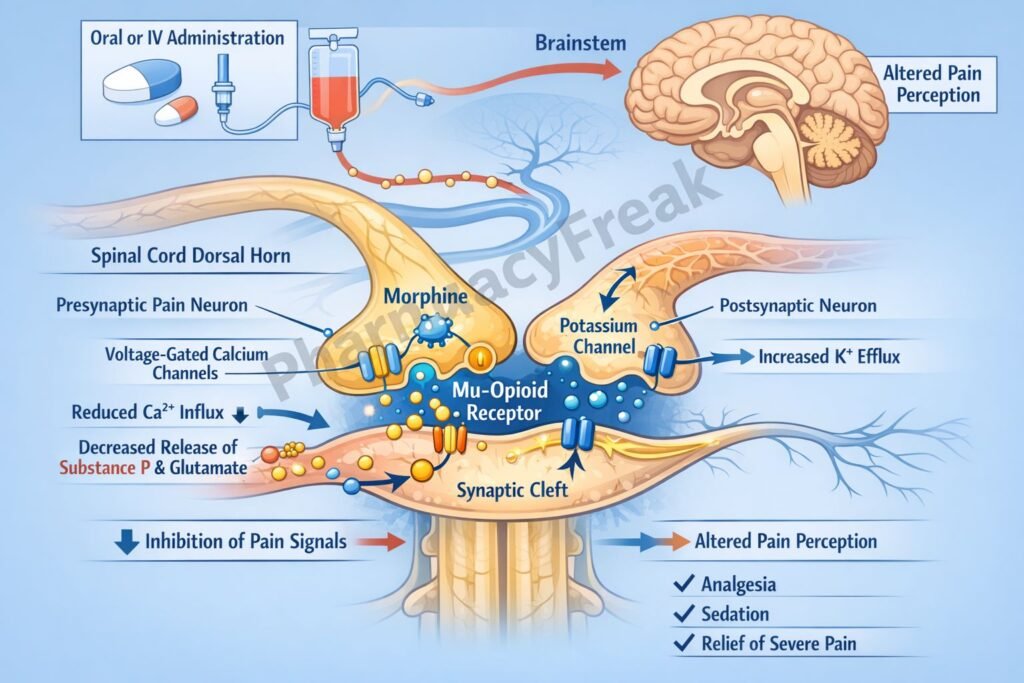
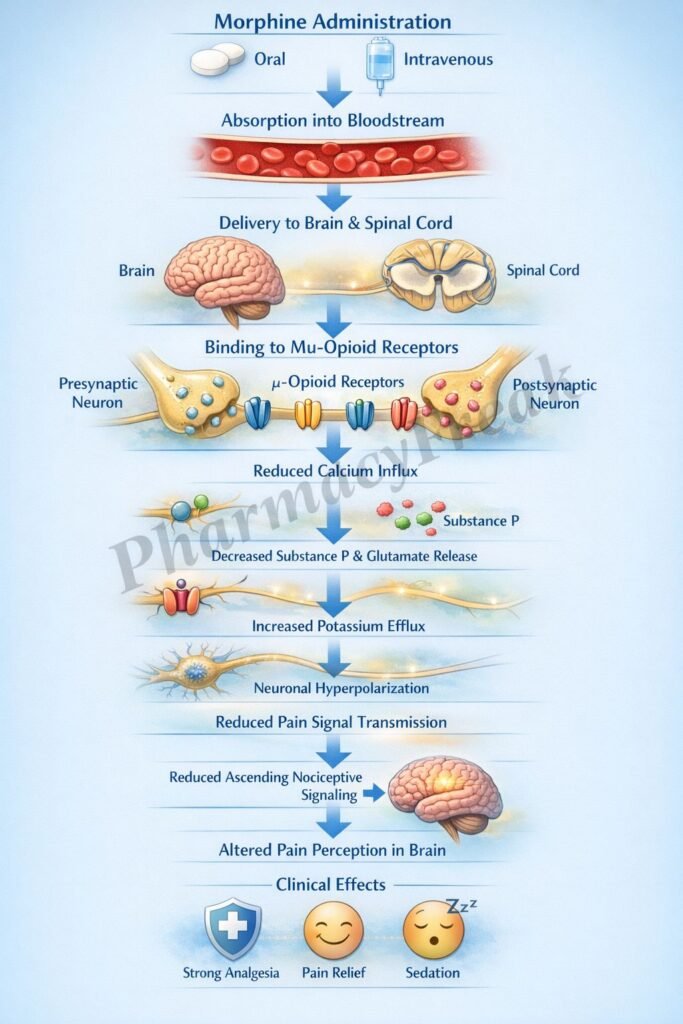
- Morphine binds to μ-opioid receptors (MOR) in the brain and spinal cord.
- These receptors are G-protein coupled (Gi/o type).
- Activation inhibits adenylate cyclase activity.
- This reduces intracellular cyclic AMP (cAMP) levels.
- Morphine opens potassium channels, causing K⁺ efflux.
- This leads to hyperpolarization of neurons.
- It also closes voltage-gated calcium channels (↓ Ca²⁺ influx).
- Reduced calcium entry decreases release of excitatory neurotransmitters such as glutamate, substance P, and CGRP.
- This inhibits transmission of pain signals in the dorsal horn of the spinal cord.
- Morphine also enhances descending inhibitory pain pathways from the brainstem.
- The overall effect is decreased perception and transmission of pain (analgesia).
A key exam point is that morphine is a μ-opioid receptor agonist that decreases neurotransmitter release and neuronal excitability.
Pharmacokinetics
Morphine can be administered orally, intravenously, intramuscularly, or subcutaneously. It undergoes significant first-pass metabolism, resulting in moderate oral bioavailability. It is metabolized in the liver to active metabolites such as morphine-6-glucuronide. It has a relatively short half-life and requires repeated dosing. Elimination occurs mainly via the kidneys, and accumulation may occur in renal impairment.
Clinical Uses
Morphine is used in the management of severe acute and chronic pain, including postoperative pain, cancer pain, and trauma. It is also used in myocardial infarction to relieve pain and reduce anxiety. In acute pulmonary edema, morphine helps reduce preload and improve symptoms of dyspnea. It is a cornerstone drug in palliative care.
Adverse Effects
Common adverse effects include respiratory depression, sedation, constipation, nausea, vomiting, and miosis. It can cause tolerance and physical dependence with prolonged use. Histamine release may lead to hypotension, flushing, and itching. High doses may result in respiratory arrest, which is the most serious adverse effect.
Comparative Analysis
| Feature | Morphine | Fentanyl | Methadone |
|---|---|---|---|
| Receptor activity | μ-opioid agonist | μ-opioid agonist | μ-agonist + NMDA antagonist |
| Potency | Moderate | Very high | Moderate |
| Duration | Short–moderate | Short | Long |
| Histamine release | Yes | Minimal | Minimal |
| Use | Severe pain | Anesthesia, severe pain | Pain, opioid dependence |
| Active metabolites | Yes | No | Minimal |
Morphine differs from fentanyl in having lower potency and higher histamine release. Compared to methadone, it lacks NMDA receptor antagonism and has a shorter duration of action.
MCQs
- Morphine acts primarily on which receptor?
a) Dopamine receptor
b) μ-opioid receptor
c) Serotonin receptor
d) Histamine receptor
Answer: b) μ-opioid receptor
- Morphine inhibits adenylate cyclase, leading to:
a) Increased cAMP
b) Decreased cAMP
c) Increased ATP
d) No change
Answer: b) Decreased cAMP
- Morphine causes hyperpolarization by:
a) Sodium influx
b) Potassium efflux
c) Calcium influx
d) Chloride influx
Answer: b) Potassium efflux
- Morphine decreases neurotransmitter release by reducing:
a) Sodium
b) Calcium
c) Potassium
d) Chloride
Answer: b) Calcium
- Morphine inhibits release of:
a) Insulin
b) Substance P
c) Thyroxine
d) Cortisol
Answer: b) Substance P
- Morphine is used for:
a) Mild pain
b) Severe pain
c) Diabetes
d) Asthma
Answer: b) Severe pain
- A major adverse effect is:
a) Hypertension
b) Respiratory depression
c) Hypercalcemia
d) Hypoglycemia
Answer: b) Respiratory depression
- Morphine causes:
a) Mydriasis
b) Miosis
c) No change in pupils
d) Diplopia
Answer: b) Miosis
- Morphine is metabolized in the:
a) Kidney
b) Liver
c) Lung
d) Brain
Answer: b) Liver
- Morphine may cause:
a) Hyperactivity
b) Sedation
c) Hypercalcemia
d) Tachycardia
Answer: b) Sedation
- Compared to fentanyl, morphine is:
a) More potent
b) Less potent
c) Equal potency
d) No effect
Answer: b) Less potent
- Morphine dependence is due to:
a) Renal effects
b) CNS action
c) Hepatic metabolism
d) Protein binding
Answer: b) CNS action
FAQs
What is the mechanism of action of morphine?
It activates μ-opioid receptors, decreasing neuronal excitability and neurotransmitter release.
Why does morphine cause respiratory depression?
It depresses the brainstem respiratory centers.
What is a hallmark sign of morphine overdose?
Pinpoint pupils and respiratory depression.
Does morphine cause tolerance?
Yes, especially with prolonged use.
Why does morphine cause constipation?
It reduces gastrointestinal motility.
What is its role in myocardial infarction?
It relieves pain and reduces anxiety and preload.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics – Opioids
https://accessmedicine.mhmedical.com/book.aspx?bookid=3191
Katzung: Basic and Clinical Pharmacology – Opioid Analgesics
https://accessmedicine.mhmedical.com/content.aspx?bookid=3382
Tripathi: Essentials of Medical Pharmacology – Opioids
https://www.jaypeedigital.com
Harrison’s Principles of Internal Medicine – Pain Management
https://accessmedicine.mhmedical.com

