Table of Contents
Introduction
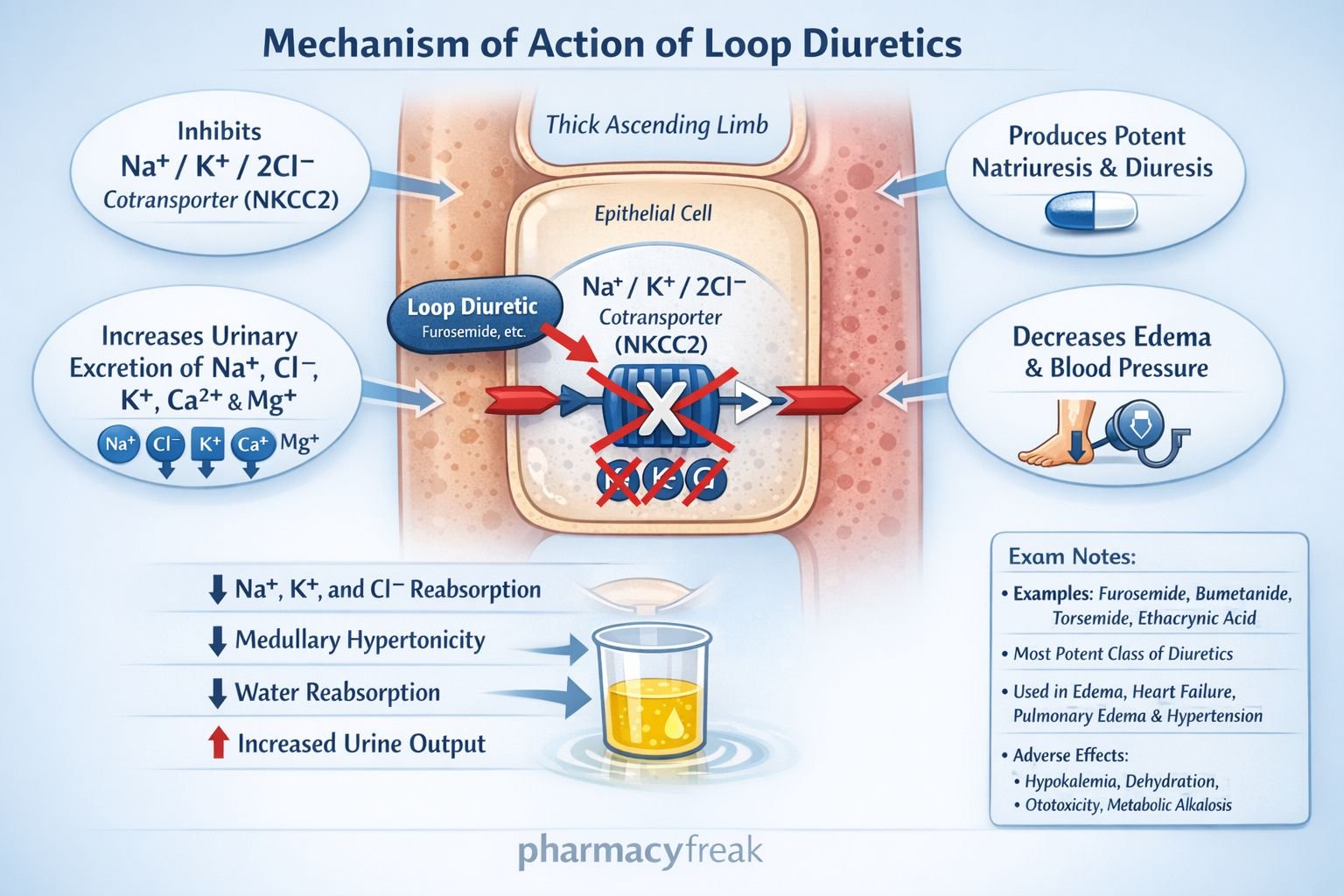
Loop diuretics are potent diuretics primarily used in conditions requiring rapid and effective removal of excess fluid, such as heart failure, pulmonary edema, and edema associated with renal or hepatic disease. The most commonly used loop diuretic is furosemide. These drugs act on the thick ascending limb of the loop of Henle and are known for their ability to produce high-ceiling diuresis. Their primary mechanism involves inhibition of sodium, potassium, and chloride reabsorption, leading to profound natriuresis and diuresis.
Mechanism of Action (Step-wise)
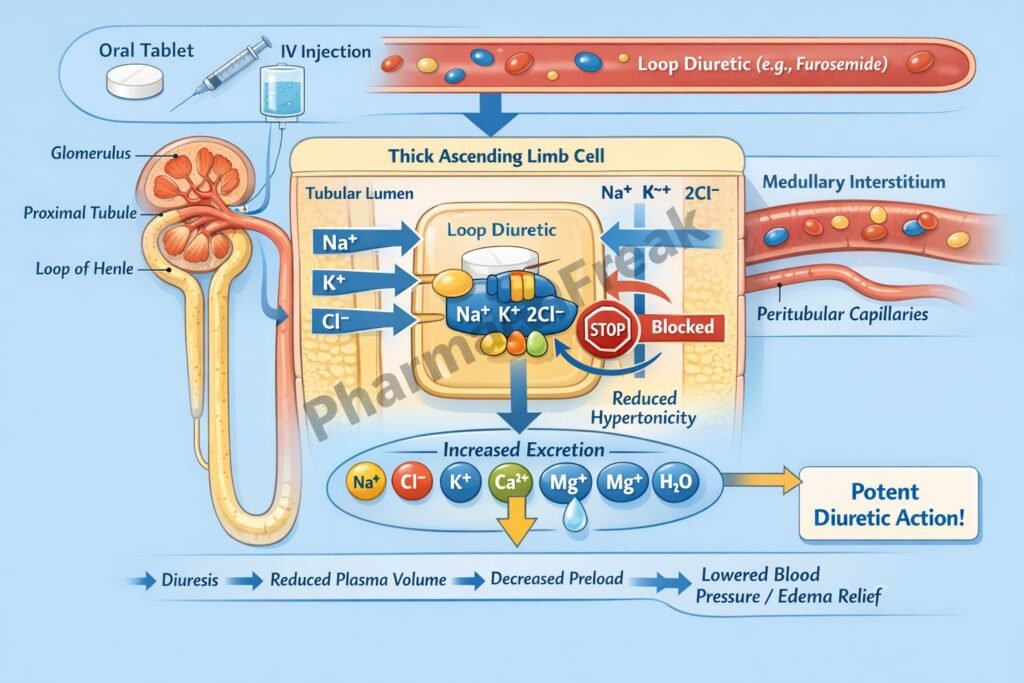
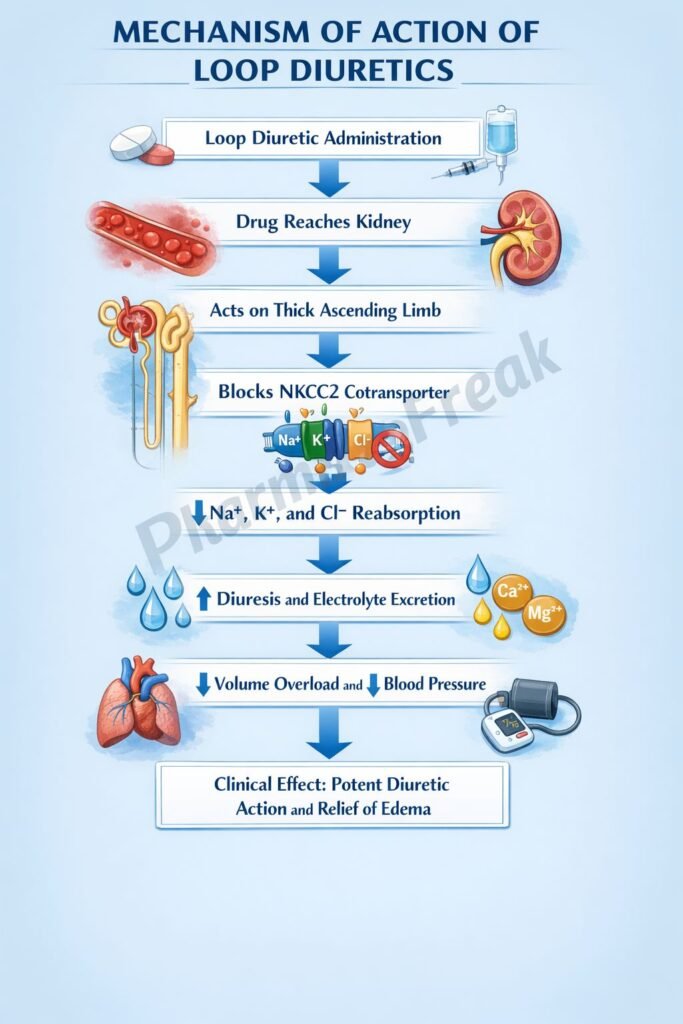
- Loop diuretics are actively secreted into the proximal tubule and reach the lumen of the nephron.
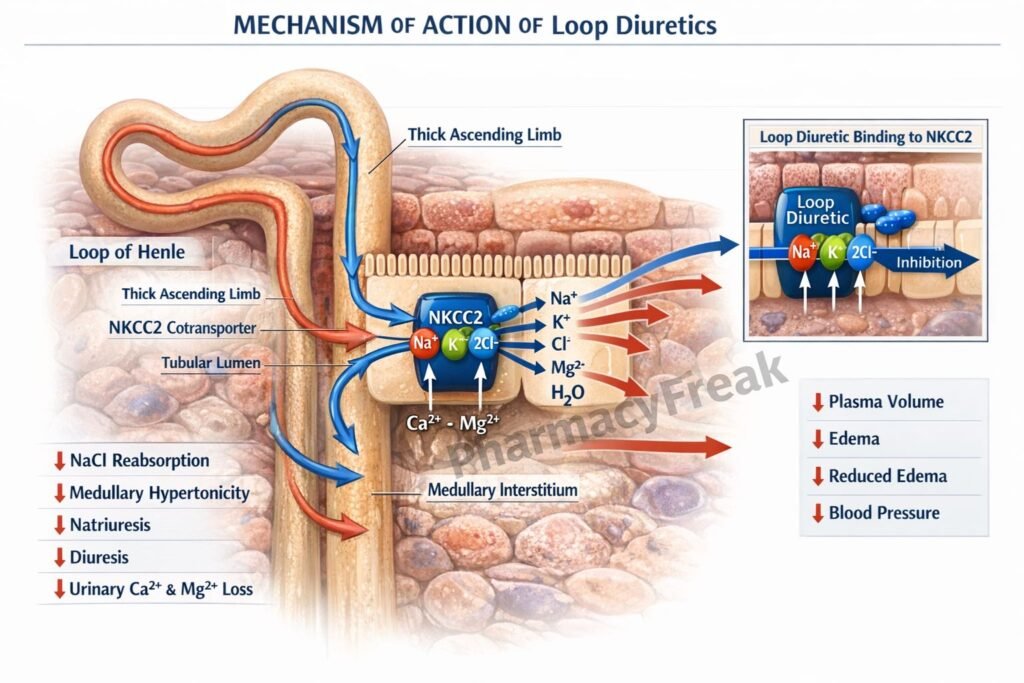
- They act on the thick ascending limb of the loop of Henle.
- They inhibit the Na⁺/K⁺/2Cl⁻ cotransporter (NKCC2) located on the luminal membrane.
- This blocks reabsorption of sodium, potassium, and chloride ions.
- Reduced solute reabsorption decreases medullary hypertonicity.
- This impairs water reabsorption in the collecting ducts.
- Increased excretion of sodium leads to increased water excretion (diuresis).
- Loss of potassium and calcium also occurs due to disruption of electrochemical gradients.
- Loop diuretics also increase renal prostaglandin synthesis, contributing to vasodilation and increased renal blood flow.
A key exam concept is that loop diuretics abolish the medullary concentration gradient, making them the most potent diuretics available.
Pharmacokinetics
Loop diuretics such as furosemide, bumetanide, and torsemide are administered orally or intravenously. They are highly protein-bound and are secreted into the proximal tubule via organic acid transporters. Their onset is rapid, especially when given intravenously. Duration varies depending on the drug, with furosemide having a shorter duration compared to torsemide. They are eliminated primarily by the kidneys, although some hepatic metabolism occurs with certain agents.
Clinical Uses
Loop diuretics are used in a variety of clinical conditions requiring rapid fluid removal. These include acute pulmonary edema, congestive heart failure, nephrotic syndrome, and cirrhosis with ascites. They are also used in hypertension, especially when associated with renal impairment. Additionally, loop diuretics are used to treat hypercalcemia because they increase calcium excretion.
Adverse Effects
Loop diuretics can cause several electrolyte disturbances, including hypokalemia, hyponatremia, hypomagnesemia, and hypocalcemia. Volume depletion and hypotension are also common. Ototoxicity is a notable adverse effect, especially with high doses or rapid intravenous administration. Hyperuricemia may occur, leading to gout. Metabolic alkalosis can develop due to increased hydrogen ion loss.
Comparative Analysis
| Feature | Loop Diuretics | Thiazide Diuretics | Potassium-Sparing Diuretics |
|---|---|---|---|
| Site of action | Thick ascending limb | Distal convoluted tubule | Collecting duct |
| Transporter inhibited | NKCC2 (Na⁺/K⁺/2Cl⁻) | Na⁺/Cl⁻ cotransporter | Aldosterone receptor or ENaC |
| Potency | High (high ceiling) | Moderate | Low |
| Effect on calcium | Increased excretion | Decreased excretion | Minimal effect |
| Major use | Edema, pulmonary edema | Hypertension | Prevent hypokalemia |
| Risk of hypokalemia | High | Moderate | Low |
Loop diuretics are the most potent diuretics and are preferred in severe fluid overload states. Thiazides are less potent and commonly used in hypertension, while potassium-sparing diuretics are mainly used to prevent potassium loss.
MCQs
- Loop diuretics act on which part of the nephron?
a) Proximal tubule
b) Thick ascending limb
c) Distal tubule
d) Collecting duct
Answer: b) Thick ascending limb
- The primary transporter inhibited by loop diuretics is:
a) Na⁺/Cl⁻
b) Na⁺/K⁺/2Cl⁻
c) Na⁺/H⁺
d) Ca²⁺ channel
Answer: b) Na⁺/K⁺/2Cl⁻
- Loop diuretics decrease reabsorption of:
a) Sodium only
b) Sodium and potassium
c) Sodium, potassium, and chloride
d) Glucose
Answer: c) Sodium, potassium, and chloride
- Loop diuretics increase excretion of:
a) Calcium
b) Glucose
c) Amino acids
d) Bicarbonate only
Answer: a) Calcium
- A major adverse effect is:
a) Hyperkalemia
b) Hypokalemia
c) Hypercalcemia
d) Hypernatremia
Answer: b) Hypokalemia
- Which loop diuretic is most commonly used?
a) Hydrochlorothiazide
b) Furosemide
c) Spironolactone
d) Amiloride
Answer: b) Furosemide
- Loop diuretics abolish:
a) Cortical gradient
b) Medullary gradient
c) Glomerular filtration
d) Tubular secretion
Answer: b) Medullary gradient
- Which condition is treated with loop diuretics?
a) Hypercalcemia
b) Hypocalcemia
c) Hypoglycemia
d) Hyperthyroidism
Answer: a) Hypercalcemia
- Ototoxicity is associated with:
a) Low doses only
b) High doses or rapid IV use
c) Oral use only
d) Topical use
Answer: b) High doses or rapid IV use
- Loop diuretics increase prostaglandin synthesis leading to:
a) Vasoconstriction
b) Vasodilation
c) Increased aldosterone
d) Reduced GFR
Answer: b) Vasodilation
- Loop diuretics are considered:
a) Low ceiling diuretics
b) High ceiling diuretics
c) Weak diuretics
d) Osmotic diuretics
Answer: b) High ceiling diuretics
- Which electrolyte imbalance may occur?
a) Hyperkalemia
b) Hypokalemia
c) Hypermagnesemia
d) Hypercalcemia
Answer: b) Hypokalemia
FAQs
What is the main mechanism of action of loop diuretics?
They inhibit the Na⁺/K⁺/2Cl⁻ cotransporter in the thick ascending limb, leading to increased excretion of sodium and water.
Why are loop diuretics called high-ceiling diuretics?
They produce a large amount of diuresis compared to other classes.
Why do loop diuretics cause hypokalemia?
Increased sodium delivery to distal nephron enhances potassium excretion.
Why do loop diuretics increase calcium excretion?
They disrupt the electrochemical gradient required for calcium reabsorption.
What is the role of prostaglandins in loop diuretics?
They increase renal blood flow and contribute to diuretic action.
When are loop diuretics preferred over thiazides?
In severe edema or renal impairment due to their high potency.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics – Diuretics
https://accessmedicine.mhmedical.com/book.aspx?bookid=3191
Katzung: Basic and Clinical Pharmacology – Diuretics
https://accessmedicine.mhmedical.com/content.aspx?bookid=3382
Tripathi: Essentials of Medical Pharmacology – Diuretics
https://www.jaypeedigital.com
Harrison’s Principles of Internal Medicine – Fluid and Electrolyte Disorders
https://accessmedicine.mhmedical.com


