Table of Contents
Introduction
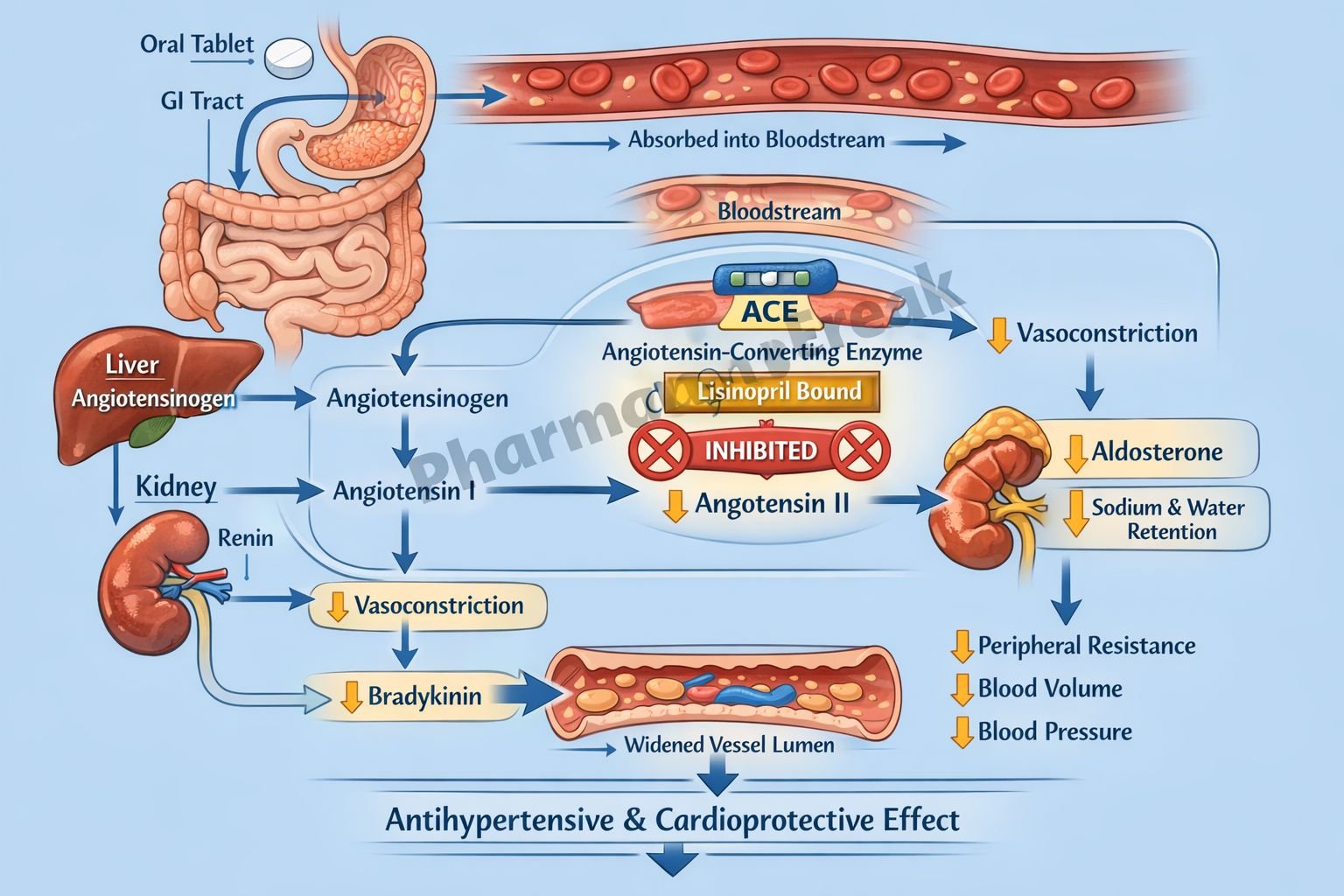
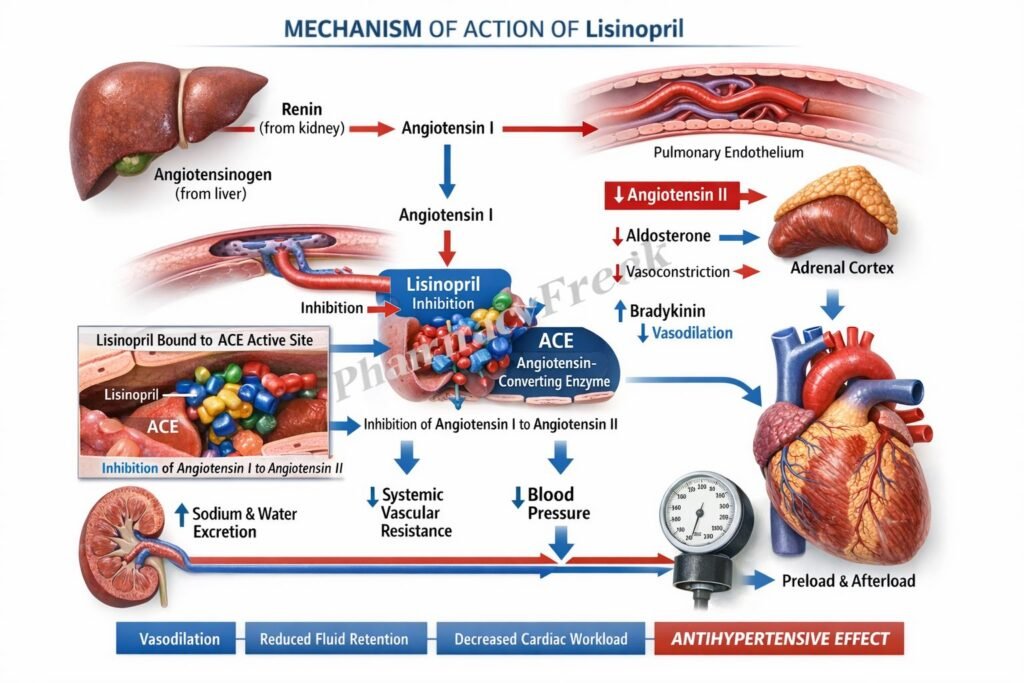
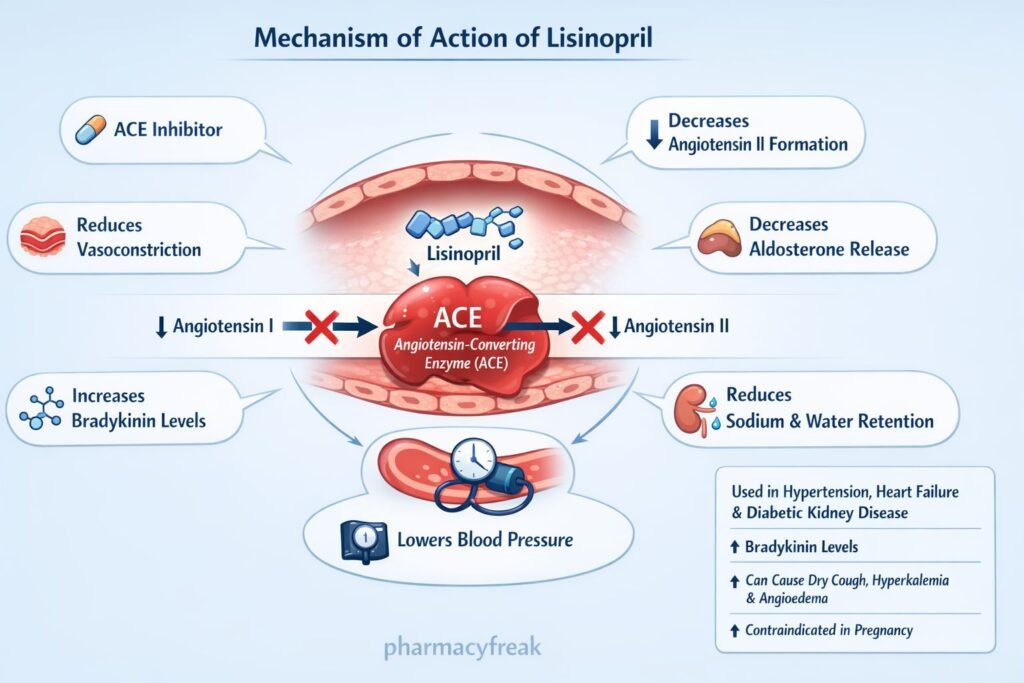
Lisinopril is a long-acting angiotensin-converting enzyme (ACE) inhibitor used mainly in hypertension, heart failure, and selected patients after acute myocardial infarction. It acts primarily by suppressing the renin-angiotensin-aldosterone system (RAAS), thereby reducing vasoconstriction, aldosterone release, and maladaptive cardiovascular remodeling. Because ACE is also involved in bradykinin breakdown, lisinopril may increase bradykinin levels, which contributes to vasodilation but also explains adverse effects such as dry cough and, rarely, angioedema.
Mechanism of Action (Step-wise)
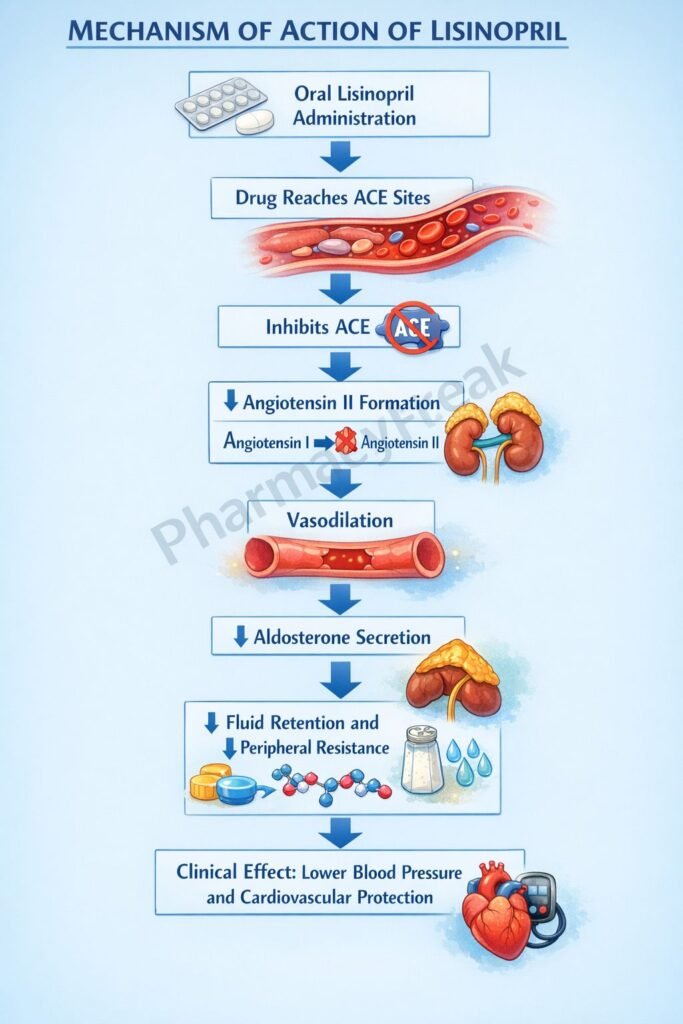
- Lisinopril inhibits angiotensin-converting enzyme in plasma and vascular endothelium.
- This reduces the conversion of angiotensin I to angiotensin II.
- Lower angiotensin II levels decrease arteriolar vasoconstriction, which lowers systemic vascular resistance and blood pressure.
- Reduced angiotensin II also decreases aldosterone secretion from the adrenal cortex.
- Lower aldosterone decreases sodium and water retention, thereby reducing preload and blood pressure.
- Loss of angiotensin II feedback increases plasma renin activity.
- Because ACE is identical to kininase II, lisinopril also reduces bradykinin degradation, which may further promote vasodilation.
- In heart failure and post myocardial infarction states, these effects reduce afterload, limit adverse ventricular remodeling, and improve hemodynamic function.
Clinically, the most important takeaway is that lisinopril does not directly block the angiotensin II receptor. Instead, it decreases angiotensin II generation upstream. This distinction is important in exams when comparing ACE inhibitors with angiotensin receptor blockers such as losartan.
Pharmacokinetics
Lisinopril is administered orally and is a long-acting ACE inhibitor. Peak serum concentrations occur about 7 hours after administration. Unlike several other ACE inhibitors, lisinopril is not a prodrug. It is not significantly metabolized and is excreted unchanged in urine. Food does not significantly affect its absorption. Its effective half-life of accumulation is about 12 hours, supporting once-daily dosing in many patients. Since elimination is predominantly renal, dose adjustment becomes important in significant renal impairment, particularly when creatinine clearance falls to 30 mL/min or below. Lisinopril is also removable by hemodialysis.
These pharmacokinetic features make lisinopril especially easy to remember for exams: oral, active as given, unchanged renal excretion, and caution in renal dysfunction.
Clinical Uses
Lisinopril is indicated for hypertension in adults and in pediatric patients 6 years and older. It is also used as adjunct therapy in heart failure and in selected patients with acute myocardial infarction. In broader clinical practice, ACE inhibitors are especially valued in hypertensive patients with diabetes, proteinuric kidney disease, or reduced ejection fraction because they lower blood pressure while offering cardiorenal benefits.
Important clinical uses include:
Hypertension: lowers systemic vascular resistance with little change in cardiac output.
Heart failure: reduces preload and afterload, improves symptoms, and slows progression.
Post myocardial infarction: helps limit ventricular remodeling and improves outcomes in appropriate patients.
Diabetic or proteinuric kidney disease: reduces intraglomerular pressure and slows progression of renal damage.
Adverse Effects
The common adverse effects of lisinopril include dry cough, hypotension, dizziness, and hyperkalemia. Dry cough is related to reduced bradykinin degradation and is a classic exam point for ACE inhibitors. Hyperkalemia occurs because aldosterone secretion falls, reducing potassium excretion.
A serious but less common adverse effect is angioedema, which can involve the face, lips, tongue, glottis, or larynx and may become life-threatening. Renal dysfunction can also occur, particularly in patients with renal artery stenosis, severe heart failure, or pre-existing renal impairment. ACE inhibitors are contraindicated in pregnancy because drugs acting directly on the renin-angiotensin system can cause fetal injury and death, especially during the second and third trimesters.
In exams, lisinopril is commonly contrasted with angiotensin receptor blockers. Both can cause hyperkalemia and are contraindicated in pregnancy, but cough and angioedema are more strongly associated with ACE inhibitors because of bradykinin accumulation.
Comparative Analysis
| Feature | Lisinopril | Enalapril | Losartan |
|---|---|---|---|
| Drug class | ACE inhibitor | ACE inhibitor | ARB |
| Prodrug status | Not a prodrug | Prodrug converted to enalaprilat | Active drug |
| Primary target | ACE inhibition | ACE inhibition | AT1 receptor blockade |
| Effect on bradykinin | Increases bradykinin | Increases bradykinin | No bradykinin increase |
| Dry cough risk | Commoner than ARBs | Commoner than ARBs | Lower risk |
| Angioedema risk | Present | Present | Lower than ACE inhibitors |
| Use in hypertension | Yes | Yes | Yes |
| Use in heart failure | Yes | Yes | Used when ACE inhibitor not tolerated |
| Pregnancy | Contraindicated | Contraindicated | Contraindicated |
Lisinopril and enalapril share the same class effect because both inhibit ACE, but lisinopril is active as administered, whereas enalapril is a prodrug. Losartan differs by blocking the angiotensin II receptor rather than ACE, so it does not increase bradykinin and is less likely to produce cough. This is the key comparison commonly tested in pharmacology exams.
MCQs
- Lisinopril belongs to which class of drugs?
a) Beta blockers
b) ACE inhibitors
c) Calcium channel blockers
d) Loop diuretics
Answer: b) ACE inhibitors
- The primary molecular action of lisinopril is:
a) Blockade of AT1 receptors
b) Inhibition of renin release
c) Inhibition of angiotensin-converting enzyme
d) Blockade of aldosterone receptors
Answer: c) Inhibition of angiotensin-converting enzyme
- Lisinopril decreases blood pressure mainly by reducing formation of:
a) Angiotensin I
b) Renin
c) Bradykinin
d) Angiotensin II
Answer: d) Angiotensin II
- Which hormone decreases secondary to lisinopril therapy?
a) Cortisol
b) Aldosterone
c) Insulin
d) Thyroxine
Answer: b) Aldosterone
- Dry cough with lisinopril is most closely related to increased:
a) Dopamine
b) Histamine
c) Bradykinin
d) Acetylcholine
Answer: c) Bradykinin
- Which of the following best describes lisinopril pharmacokinetics?
a) It is extensively metabolized in the liver
b) It is a prodrug
c) It is excreted unchanged in urine
d) Food completely blocks its absorption
Answer: c) It is excreted unchanged in urine
- Lisinopril is commonly used in all of the following except:
a) Hypertension
b) Heart failure
c) Acute myocardial infarction in selected patients
d) Bronchial asthma relief
Answer: d) Bronchial asthma relief
- A major electrolyte abnormality associated with lisinopril is:
a) Hypokalemia
b) Hyperkalemia
c) Hypocalcemia
d) Hypernatremia
Answer: b) Hyperkalemia
- Which adverse effect of lisinopril can become life-threatening?
a) Constipation
b) Tinnitus
c) Angioedema
d) Mydriasis
Answer: c) Angioedema
- Lisinopril is contraindicated in:
a) Pregnancy
b) Hyperthyroidism
c) Migraine
d) Peptic ulcer disease
Answer: a) Pregnancy
- Compared with losartan, lisinopril is more likely to cause:
a) Dry cough
b) Severe sedation
c) Hypoglycemia
d) Constipation
Answer: a) Dry cough
- The effect of lisinopril on the renin-angiotensin-aldosterone system leads to:
a) Increased vasoconstriction
b) Increased sodium retention
c) Reduced afterload
d) Increased aldosterone secretion
Answer: c) Reduced afterload
FAQs
What is the main mechanism of action of lisinopril?
Lisinopril inhibits ACE, reducing conversion of angiotensin I to angiotensin II and thereby lowering vasoconstriction and aldosterone secretion.
Why does lisinopril cause cough?
It can increase bradykinin levels because ACE also functions as kininase II, an enzyme involved in bradykinin degradation.
Is lisinopril a prodrug?
No. Lisinopril is active in the administered form and does not require metabolic activation.
Can lisinopril be used in kidney disease?
Yes, it is often useful in proteinuric renal disease, but renal function and potassium must be monitored carefully, especially in impaired renal function.
Why is lisinopril contraindicated in pregnancy?
Drugs acting on the renin-angiotensin system can injure or even kill the developing fetus.
How is lisinopril different from ARBs?
Lisinopril inhibits ACE, whereas ARBs block angiotensin II receptors. ARBs generally have less cough because they do not increase bradykinin to the same extent.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics – Book Page
Katzung’s Basic & Clinical Pharmacology – Antihypertensive Agents


