Table of Contents
Introduction
GLP-1 analogues, also known as GLP-1 receptor agonists, are an important class of antidiabetic drugs used in the management of type 2 diabetes mellitus and obesity. These drugs mimic the action of the endogenous incretin hormone glucagon-like peptide-1 (GLP-1), which is secreted from intestinal L-cells after food intake.
GLP-1 analogues enhance glucose dependent insulin secretion, suppress glucagon release, slow gastric emptying, and promote satiety. Because their action depends on blood glucose levels, they have a lower risk of hypoglycemia compared with sulfonylureas.
Common examples include liraglutide, semaglutide, exenatide, dulaglutide, and lixisenatide. Their mechanisms are frequently tested in pharmacology examinations such as USMLE, NEET PG, FMGE, PLAB, INICET, NCLEX, and MCCQE.
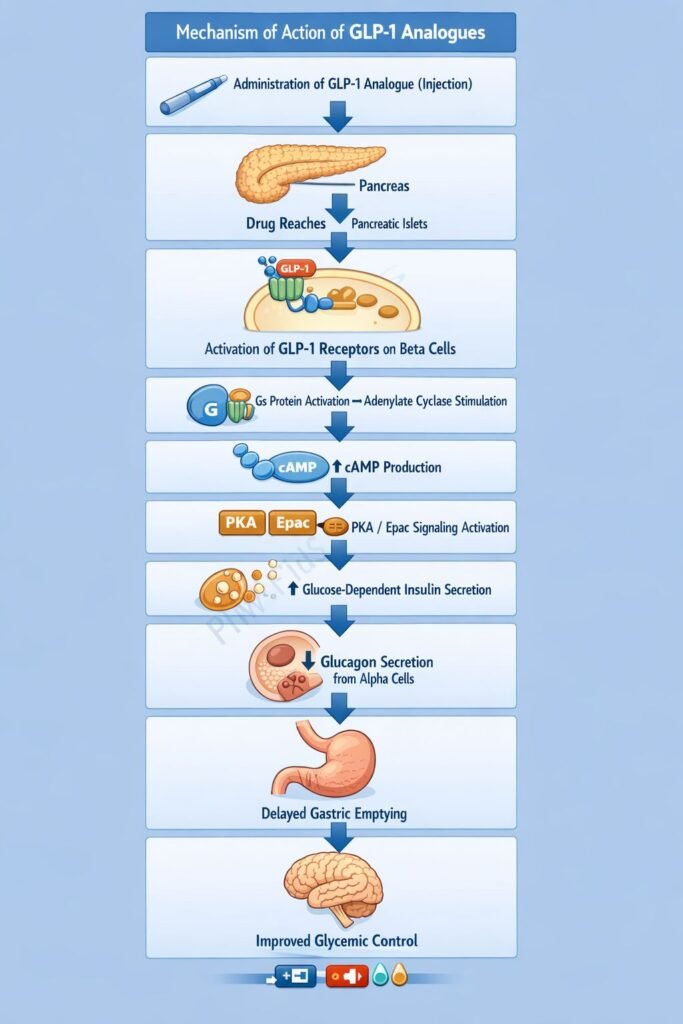
Mechanism of Action (Step-wise)
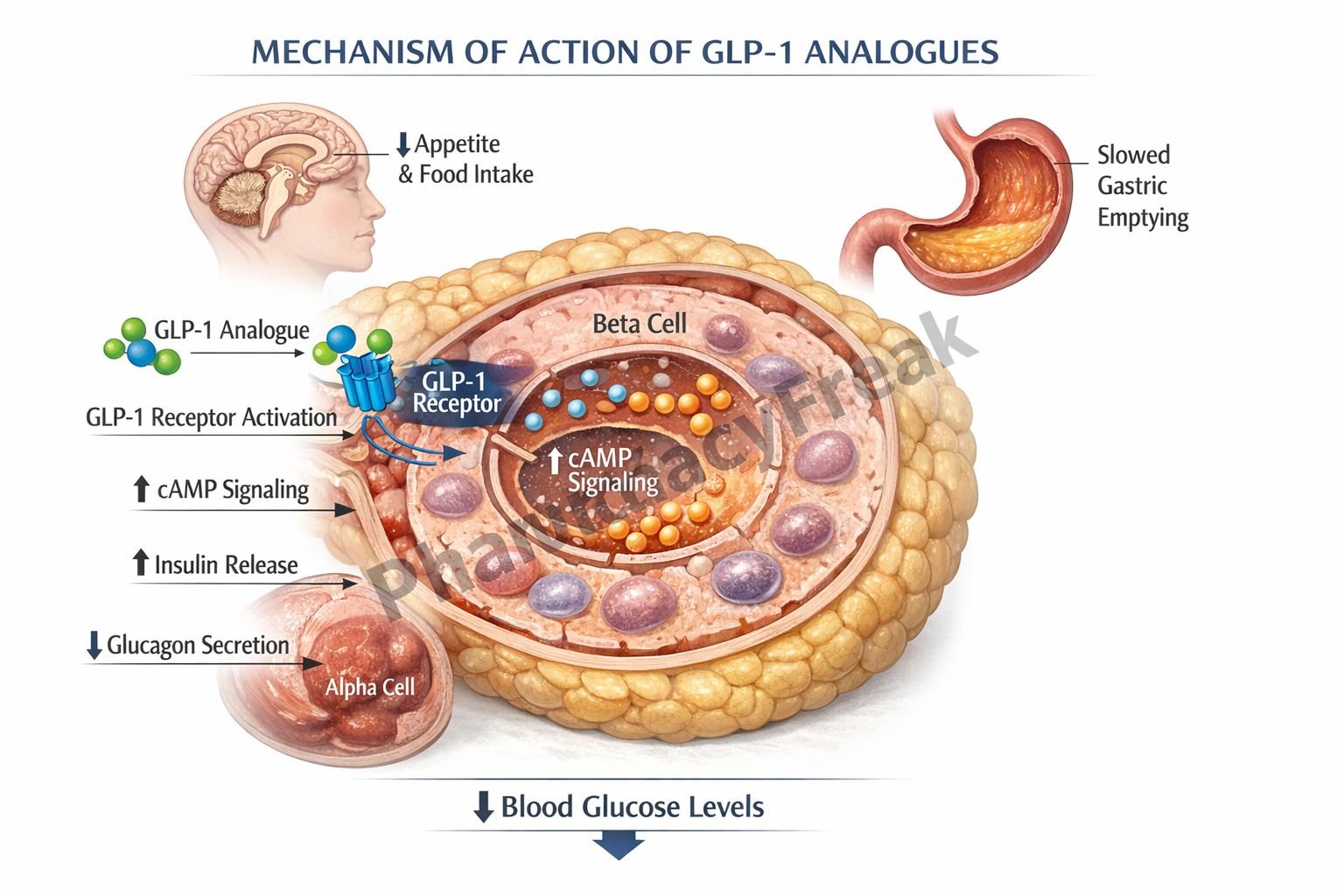
GLP-1 analogues mimic the incretin hormone GLP-1 and activate GLP-1 receptors in multiple organs.
Step 1: Activation of GLP-1 receptors
GLP-1 analogues bind to GLP-1 receptors on pancreatic beta cells, which are G protein coupled receptors.
Step 2: Increased cyclic AMP production
Receptor activation stimulates adenylate cyclase, increasing intracellular cyclic AMP levels.
Step 3: Enhanced glucose dependent insulin secretion
Elevated cAMP enhances insulin secretion from pancreatic beta cells, but only when blood glucose levels are elevated.
Step 4: Suppression of glucagon secretion
GLP-1 receptor activation inhibits glucagon release from pancreatic alpha cells, reducing hepatic glucose production.
Step 5: Delayed gastric emptying
GLP-1 analogues slow gastric emptying, reducing the rate of glucose absorption from the intestine.
Step 6: Appetite suppression
They act on hypothalamic centers to increase satiety and reduce food intake.
Overall effect:
Improved glycemic control through increased insulin secretion, decreased glucagon secretion, reduced hepatic glucose production, and delayed gastric emptying.
Important concept:
GLP-1 analogues produce glucose dependent insulin release, which significantly reduces the risk of hypoglycemia.
Pharmacokinetics
Administration:
Most GLP-1 analogues are administered via subcutaneous injection. Oral semaglutide is also available.
Absorption:
Slow absorption following subcutaneous injection.
Metabolism:
Resistant to degradation by dipeptidyl peptidase-4 (DPP-4).
Duration:
Half life varies by drug, allowing daily or weekly dosing.
Excretion:
Eliminated mainly through proteolytic degradation and renal mechanisms.
Clinical Uses
- Type 2 diabetes mellitus
- Weight management in obese or overweight patients
- Reduction of cardiovascular risk in high risk diabetic patients
- Combination therapy with metformin or other antidiabetic agents
These agents are particularly beneficial in patients requiring weight loss or cardiovascular risk reduction.
Adverse Effects
Common adverse effects:
- Nausea
- Vomiting
- Diarrhea
Less common adverse effects:
- Pancreatitis
- Injection site reactions
Precautions:
- Avoid in patients with severe gastrointestinal disease
- Contraindicated in patients with medullary thyroid carcinoma or MEN2 syndrome for certain agents
Comparative Analysis
| Feature | GLP-1 Analogues | DPP-4 Inhibitors | Sulfonylureas |
|---|---|---|---|
| Mechanism | GLP-1 receptor agonist | Prevent GLP-1 breakdown | Stimulate insulin secretion |
| Insulin release | Glucose dependent | Glucose dependent | Glucose independent |
| Weight effect | Weight loss | Weight neutral | Weight gain |
| Hypoglycemia risk | Low | Low | Higher |
| Route | Mostly injectable | Oral | Oral |
Explanation:
GLP-1 analogues directly activate GLP-1 receptors, producing stronger incretin effects than DPP-4 inhibitors, which simply prevent degradation of endogenous GLP-1. Sulfonylureas stimulate insulin secretion independent of glucose levels, increasing hypoglycemia risk, while GLP-1 analogues release insulin only when glucose levels are elevated.
MCQs
- GLP-1 analogues primarily act on which receptor?
a) NMDA receptor
b) GLP-1 receptor
c) PPAR gamma
d) SUR1
Answer: b) GLP-1 receptor
- GLP-1 receptor activation increases:
a) cAMP
b) cGMP
c) ATP degradation
d) Sodium influx
Answer: a) cAMP
- GLP-1 analogues stimulate insulin release in a:
a) Glucose independent manner
b) Glucose dependent manner
c) Continuous manner
d) Insulin independent manner
Answer: b) Glucose dependent manner
- Which hormone secretion is suppressed by GLP-1 analogues?
a) Insulin
b) Cortisol
c) Glucagon
d) Growth hormone
Answer: c) Glucagon
- GLP-1 analogues slow:
a) Hepatic metabolism
b) Gastric emptying
c) Renal clearance
d) Insulin degradation
Answer: b) Gastric emptying
- Which effect contributes to weight loss?
a) Increased appetite
b) Satiety signaling
c) Increased glucagon
d) Increased glycogenolysis
Answer: b) Satiety signaling
- Common adverse effect:
a) Hypertension
b) Nausea
c) Hyperkalemia
d) Bradycardia
Answer: b) Nausea
- GLP-1 analogues are resistant to degradation by:
a) MAO
b) COMT
c) DPP-4
d) CYP3A4
Answer: c) DPP-4
- Which drug class also acts on incretin pathway?
a) DPP-4 inhibitors
b) Sulfonylureas
c) Thiazolidinediones
d) SGLT2 inhibitors
Answer: a) DPP-4 inhibitors
- Major advantage of GLP-1 analogues over sulfonylureas:
a) Higher hypoglycemia risk
b) Glucose dependent insulin release
c) No insulin secretion
d) Increased glucagon release
Answer: b) Glucose dependent insulin release
FAQs
- What are GLP-1 analogues used for?
They are used to treat type 2 diabetes and obesity. - How do GLP-1 analogues lower blood glucose?
By increasing glucose dependent insulin secretion and decreasing glucagon release. - Why do GLP-1 analogues cause weight loss?
They slow gastric emptying and promote satiety. - Do GLP-1 analogues cause hypoglycemia?
They have a low risk because insulin release depends on glucose levels. - What is the difference between GLP-1 analogues and DPP-4 inhibitors?
GLP-1 analogues directly activate GLP-1 receptors, while DPP-4 inhibitors prevent breakdown of endogenous incretin hormones. - Are GLP-1 analogues injectable drugs?
Most are injectable, although oral semaglutide is available.
References
Goodman & Gilman’s Pharmacological Basis of Therapeutics
https://accessmedicine.mhmedical.com/book.aspx?bookID=2189
Katzung BG. Basic and Clinical Pharmacology
https://accessmedicine.mhmedical.com/book.aspx?bookID=2249
Tripathi KD. Essentials of Medical Pharmacology
https://jaypeedigital.com/book/9789354651970
Harrison’s Principles of Internal Medicine
https://accessmedicine.mhmedical.com/book.aspx?bookID=3095


