Table of Contents
Introduction
Fosfomycin is a broad spectrum bactericidal antibiotic primarily used in the treatment of uncomplicated urinary tract infections. It is structurally unrelated to other major antibiotic classes and represents a unique inhibitor of bacterial cell wall synthesis. Because of its distinct mechanism, fosfomycin retains activity against many multidrug resistant organisms, including ESBL producing Enterobacteriaceae and some carbapenem resistant strains.
Its mechanism of action is frequently tested in USMLE, NEET PG, FMGE, PLAB, INICET, NCLEX, and MCCQE due to its early step inhibition in peptidoglycan synthesis.
Mechanism of Action (Step-wise)
Fosfomycin inhibits bacterial cell wall synthesis at an earlier stage than beta lactams and vancomycin.
Step 1: Bacterial uptake
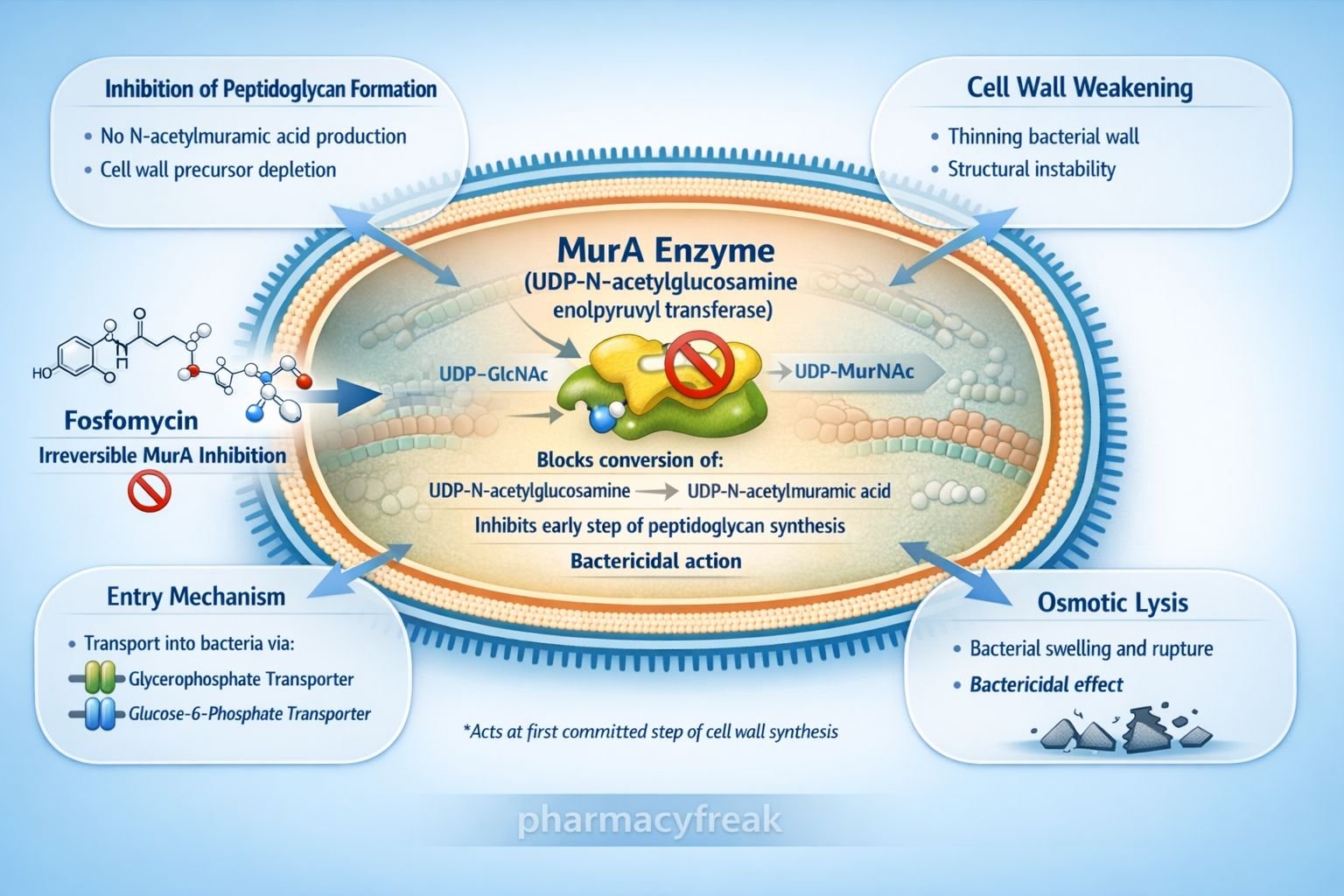
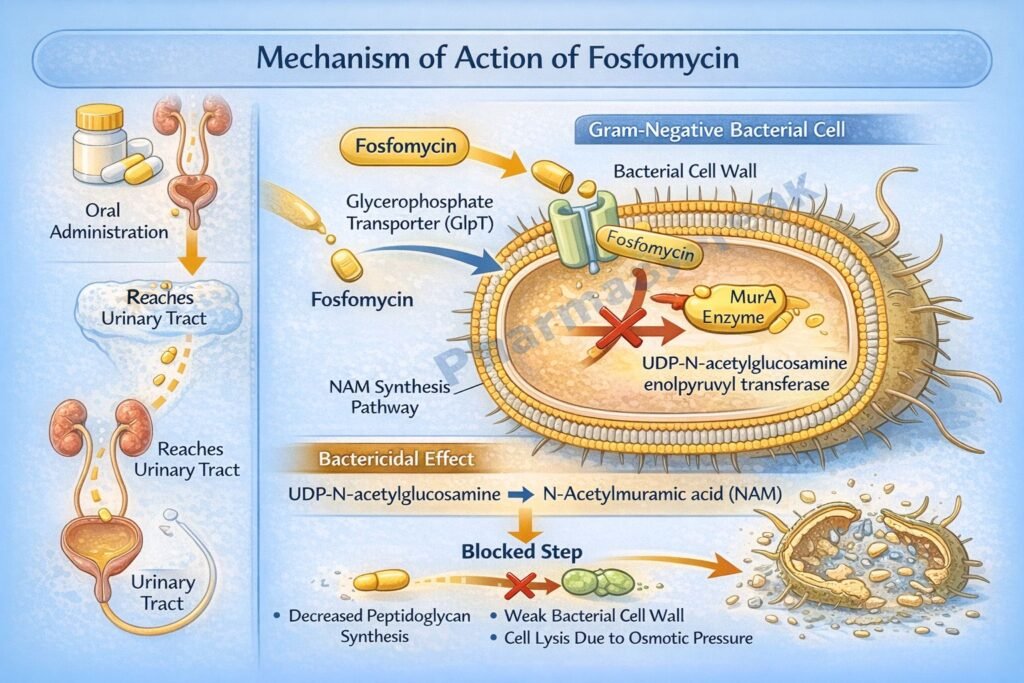
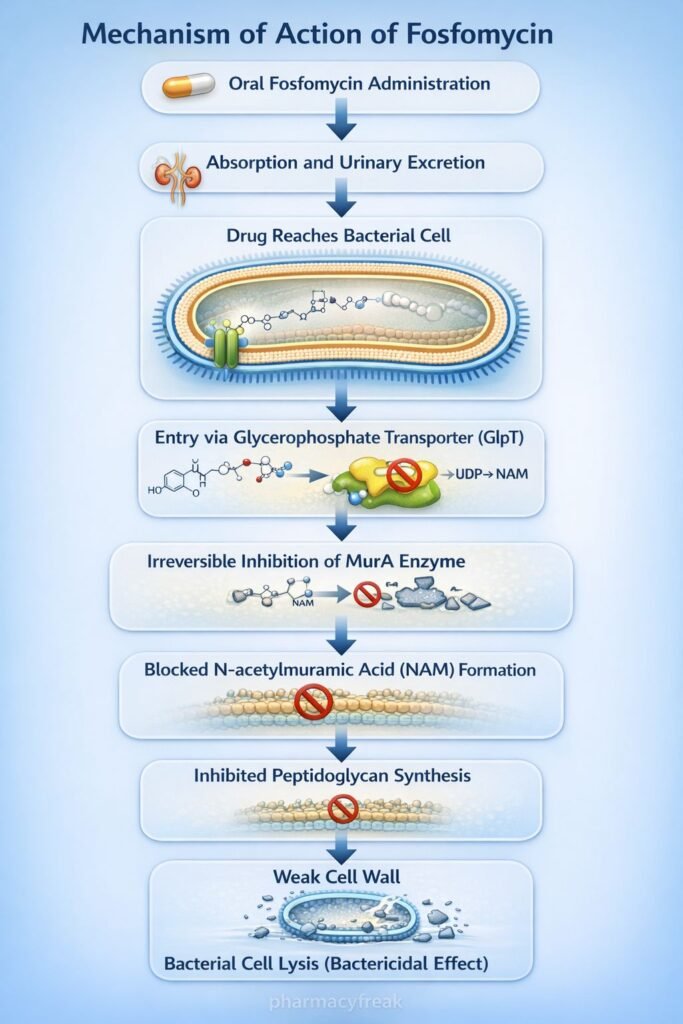
Fosfomycin enters bacterial cells via active transport systems:
- Glycerophosphate transporter
- Glucose 6 phosphate transporter
Step 2: Target enzyme binding
Inside the bacterial cytoplasm, fosfomycin irreversibly inhibits the enzyme UDP N acetylglucosamine enolpyruvyl transferase, also called MurA.
Step 3: Blockade of first committed step
MurA catalyzes the conversion of UDP N acetylglucosamine to UDP N acetylmuramic acid, the first committed step in peptidoglycan synthesis.
Step 4: Inhibition of peptidoglycan formation
By blocking MurA, fosfomycin prevents formation of N acetylmuramic acid, an essential precursor for bacterial cell wall synthesis.
Step 5: Bacterial cell lysis
Inhibition of peptidoglycan synthesis leads to weakened cell wall integrity, osmotic instability, and bacterial cell death.
Overall effect:
Bactericidal action due to inhibition of early cytoplasmic stage of cell wall synthesis.
Key exam point:
Fosfomycin acts before beta lactams, which inhibit transpeptidation, and before vancomycin, which blocks peptide cross linking.
Pharmacokinetics
Absorption:
Orally administered fosfomycin trometamol has good bioavailability. Food may reduce absorption slightly.
Distribution:
Widely distributed. Achieves very high urinary concentrations, making it effective for urinary tract infections.
Metabolism:
Minimal metabolism.
Excretion:
Excreted unchanged in urine via glomerular filtration.
Half life:
Approximately 4 to 6 hours.
Special feature:
Single dose therapy is effective for uncomplicated cystitis due to prolonged high urinary levels.
Clinical Uses
- Uncomplicated urinary tract infections, especially cystitis
- Infections caused by ESBL producing organisms
- Multidrug resistant gram negative infections
- Alternative therapy in patients allergic to beta lactams
Common pathogens covered:
- Escherichia coli
- Klebsiella species
- Enterococcus faecalis
Adverse Effects
Fosfomycin is generally well tolerated.
Common adverse effects:
- Diarrhea
- Nausea
- Headache
Rare adverse effects:
- Hypersensitivity reactions
- Vaginitis
Resistance mechanisms:
- Mutation in MurA enzyme
- Reduced uptake due to transporter mutation
Comparative Analysis
| Feature | Fosfomycin | Beta lactams | Vancomycin |
|---|---|---|---|
| Site of action | Cytoplasmic | Periplasmic | Extracellular |
| Target | MurA enzyme | Penicillin binding proteins | D Ala D Ala terminus |
| Step inhibited | Early peptidoglycan synthesis | Transpeptidation | Cross linking |
| Bactericidal | Yes | Yes | Yes |
| Use in UTI | Excellent | Variable | Limited |
Explanation:
Fosfomycin inhibits the earliest step of peptidoglycan synthesis by blocking MurA. Beta lactams act later by inhibiting penicillin binding proteins responsible for cross linking. Vancomycin binds to D Ala D Ala residues, preventing peptide cross linking. Because fosfomycin acts intracellularly and early, it is effective against certain resistant organisms.
MCQs
- Fosfomycin inhibits which enzyme?
a) Dihydrofolate reductase
b) MurA
c) Penicillin binding protein
d) DNA gyrase
Answer: b) MurA
- Fosfomycin inhibits synthesis of:
a) DNA
b) RNA
c) Peptidoglycan
d) Protein
Answer: c) Peptidoglycan
- Fosfomycin is primarily used for:
a) Pneumonia
b) Meningitis
c) Uncomplicated UTI
d) Tuberculosis
Answer: c) Uncomplicated UTI
- Mechanism class:
a) Protein synthesis inhibitor
b) Cell wall synthesis inhibitor
c) DNA synthesis inhibitor
d) Antimetabolite
Answer: b) Cell wall synthesis inhibitor
- Fosfomycin enters bacteria via:
a) Passive diffusion
b) Ribosomal channel
c) Glycerophosphate transporter
d) Porins only
Answer: c) Glycerophosphate transporter
- Fosfomycin is:
a) Bacteriostatic
b) Bactericidal
c) Fungistatic
d) Antiviral
Answer: b) Bactericidal
- Resistance may occur due to mutation in:
a) PBP
b) MurA
c) 30S subunit
d) RNA polymerase
Answer: b) MurA
- Compared to beta lactams, fosfomycin acts:
a) Later
b) At same step
c) Earlier
d) After cross linking
Answer: c) Earlier
- Fosfomycin is excreted mainly via:
a) Liver
b) Feces
c) Urine
d) Lungs
Answer: c) Urine
- High urinary concentration explains its use in:
a) Skin infection
b) Bone infection
c) UTI
d) CNS infection
Answer: c) UTI
FAQs
- Why is fosfomycin effective as a single dose for cystitis?
Because it achieves very high and sustained urinary concentrations. - Is fosfomycin safe in pregnancy?
It is generally considered safe for uncomplicated UTIs during pregnancy. - Does fosfomycin cover MRSA?
It has activity against some gram positive organisms but is mainly used for UTIs. - What makes fosfomycin unique among cell wall inhibitors?
It inhibits the earliest cytoplasmic step in peptidoglycan synthesis. - Can fosfomycin be used for complicated infections?
It may be used in resistant infections, but intravenous formulations are preferred for severe cases. - How does resistance develop?
Through mutation of MurA or reduced drug uptake.
References
Goodman & Gilman’s Pharmacological Basis of Therapeutics
https://accessmedicine.mhmedical.com/book.aspx?bookID=2189
Katzung BG. Basic and Clinical Pharmacology
https://accessmedicine.mhmedical.com/book.aspx?bookID=2249
Tripathi KD. Essentials of Medical Pharmacology
https://jaypeedigital.com/book/9789354651970
Harrison’s Principles of Internal Medicine
https://accessmedicine.mhmedical.com/book.aspx?bookID=3095


