Table of Contents
Introduction
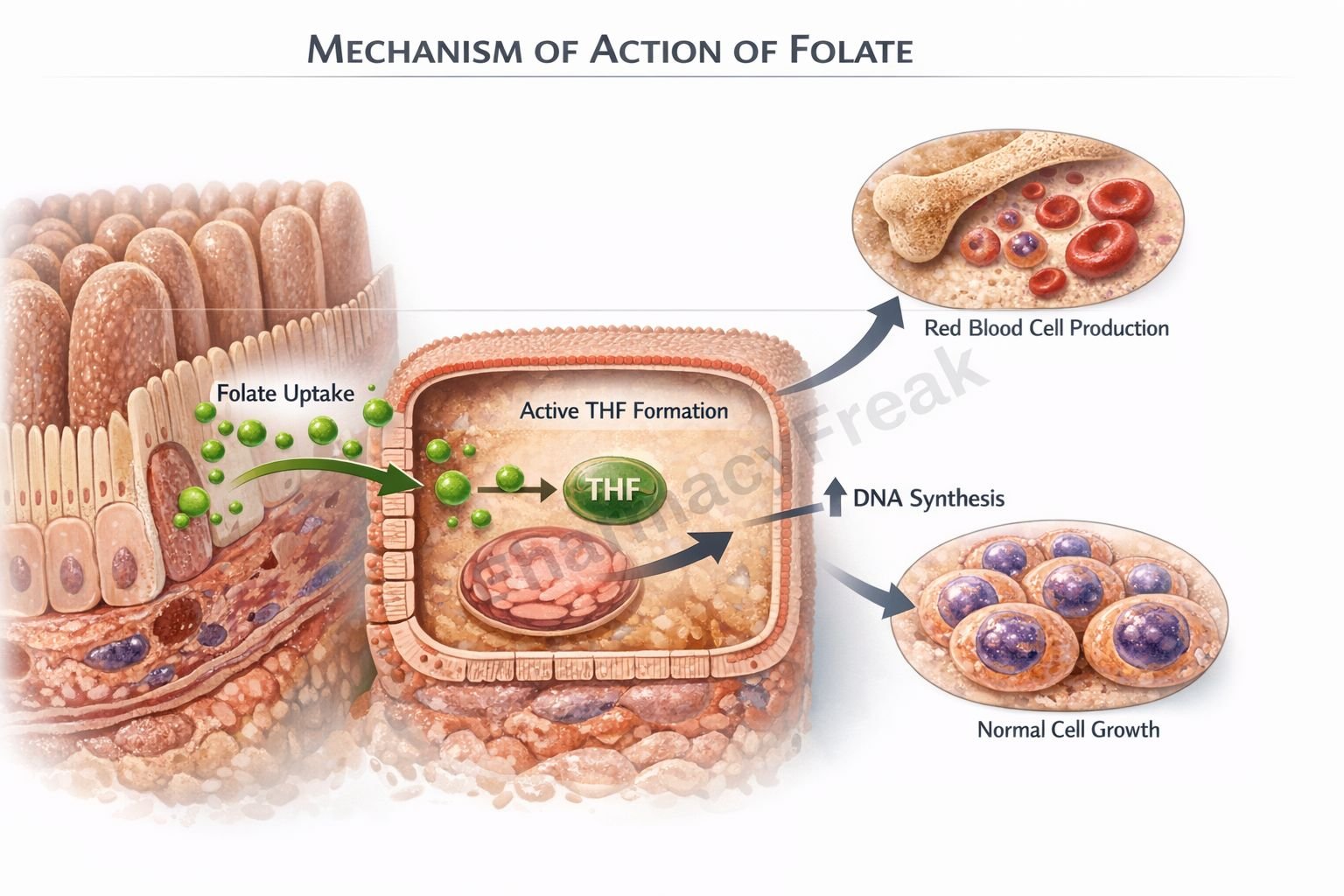
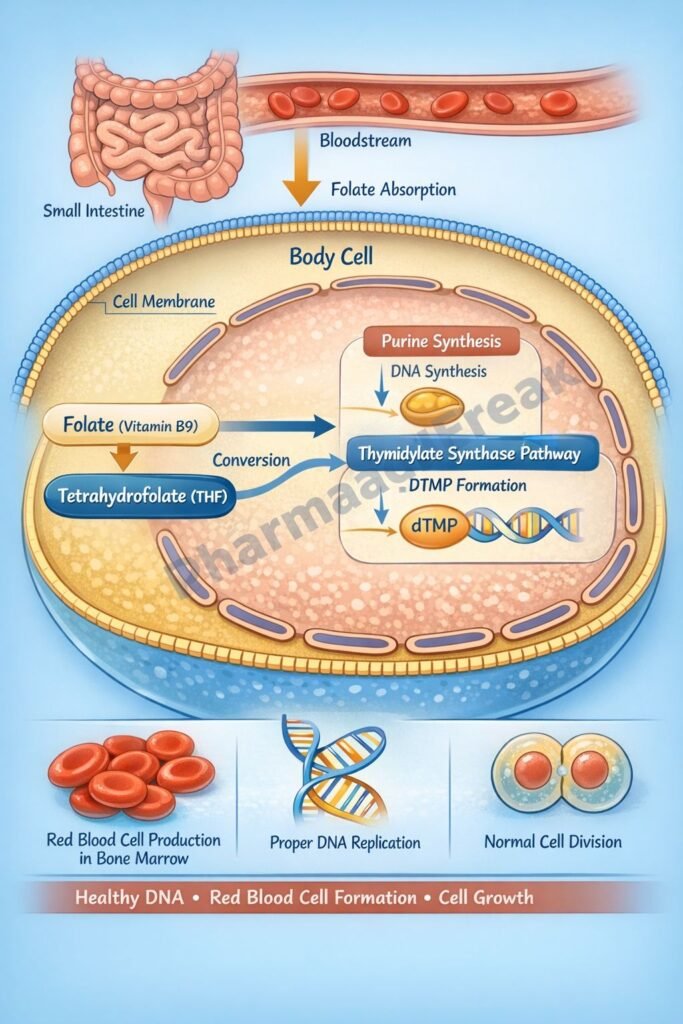
Folate, also known as vitamin B9, is a water soluble vitamin essential for DNA synthesis, cell division, and hematopoiesis. The biologically active form of folate is tetrahydrofolate, which functions as a carrier of one carbon units in multiple metabolic reactions. Folate plays a central role in nucleotide biosynthesis and methylation reactions, making it critical for rapidly dividing cells such as bone marrow and fetal tissues.
Deficiency of folate leads to impaired DNA synthesis, resulting in megaloblastic anemia and increased risk of neural tube defects during pregnancy. Understanding its mechanism of action is essential for pharmacology and clinical examinations such as USMLE, NEET PG, FMGE, PLAB, INICET, NCLEX, and MCCQE.
Mechanism of Action (Step-wise)
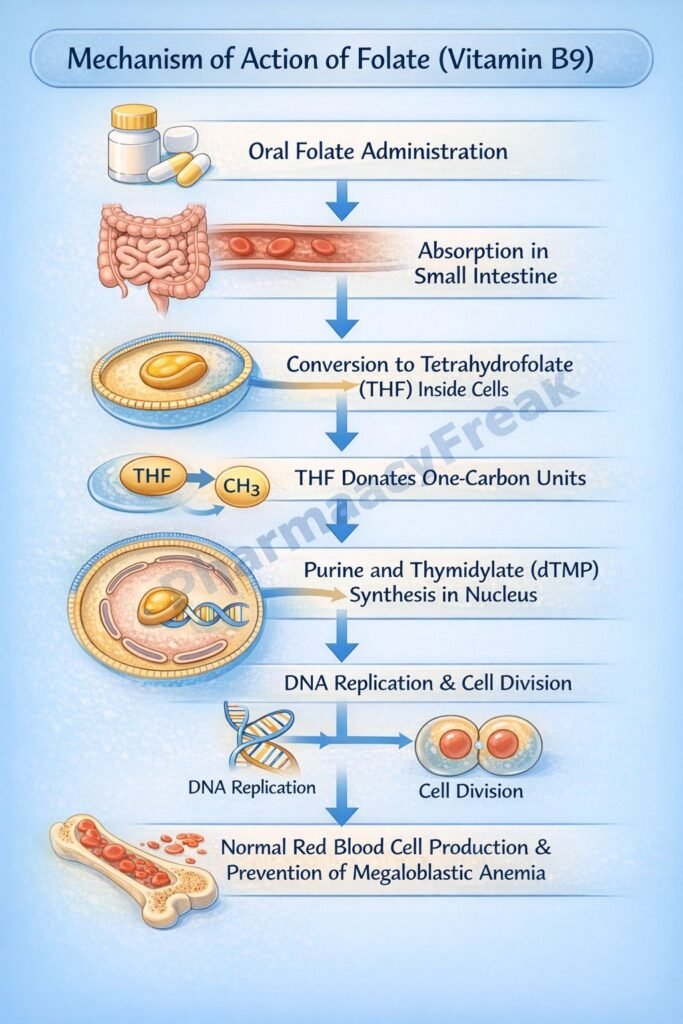
Folate acts primarily through its reduced active form, tetrahydrofolate (THF). The mechanism can be understood in the following steps:
Step 1: Conversion to active form
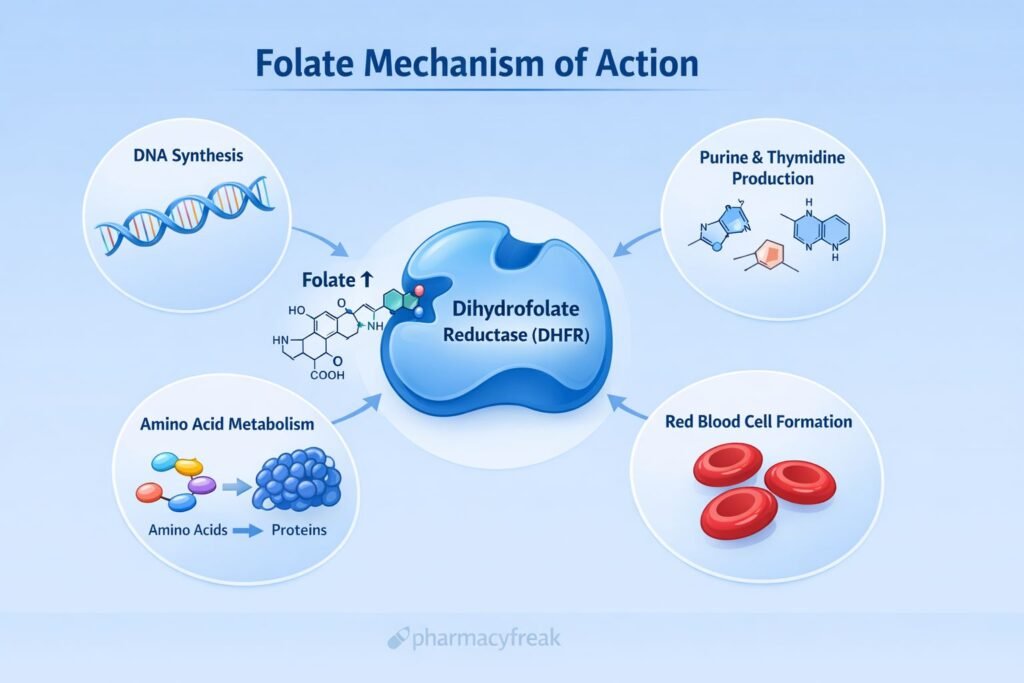
Dietary folate is converted to dihydrofolate (DHF) and then reduced by the enzyme dihydrofolate reductase (DHFR) to tetrahydrofolate (THF).
Step 2: One carbon unit transfer
THF acts as a carrier of one carbon fragments in various oxidation states. It forms derivatives such as:
- N5,N10-methylene THF
- N5-methyl THF
- N10-formyl THF
Step 3: Purine synthesis
N10-formyl THF donates one carbon units required for the synthesis of purine nucleotides (adenine and guanine).
Step 4: Thymidylate synthesis
N5,N10-methylene THF is required for the conversion of deoxyuridine monophosphate (dUMP) to deoxythymidine monophosphate (dTMP) by thymidylate synthase. This step is essential for DNA synthesis.
Step 5: Methionine synthesis
N5-methyl THF participates in the conversion of homocysteine to methionine via methionine synthase, a reaction that also requires vitamin B12. Methionine is required for S-adenosylmethionine formation, which is essential for methylation reactions.
Overall effect:
Folate enables DNA synthesis, cell replication, erythropoiesis, and methylation reactions.
Clinical pharmacology relevance:
- Folate deficiency leads to impaired DNA synthesis
- Methotrexate inhibits DHFR, blocking THF formation
- 5-fluorouracil interferes with thymidylate synthesis
- Trimethoprim inhibits bacterial DHFR
Pharmacokinetics
Absorption:
Folate is absorbed primarily in the proximal jejunum via active transport.
Distribution:
It is transported in plasma mainly as 5-methyl THF. The liver stores approximately 5 to 10 mg of folate, sufficient for about 3 to 4 months.
Metabolism:
Converted to active tetrahydrofolate derivatives in the liver.
Excretion:
Excreted mainly in urine; small amounts in bile.
Special considerations:
- Alcohol reduces absorption and storage
- Certain drugs such as methotrexate and phenytoin interfere with folate metabolism
Clinical Uses
- Treatment of megaloblastic anemia due to folate deficiency
- Prevention of neural tube defects in pregnancy
- Supplementation in chronic hemolytic anemia
- Hyperhomocysteinemia management
- Adjunct therapy in patients receiving antifolate drugs
Adverse Effects
Folate is generally safe and well tolerated.
Possible adverse effects:
- Rare allergic reactions
- Gastrointestinal upset
- High doses may mask vitamin B12 deficiency, leading to neurological damage
Important clinical warning:
Folate should not be given alone in undiagnosed megaloblastic anemia until vitamin B12 deficiency is excluded.
Comparative Analysis
| Feature | Folate | Vitamin B12 | Methotrexate |
|---|---|---|---|
| Primary role | One carbon transfer | Cofactor for methionine synthase | DHFR inhibitor |
| DNA synthesis | Required | Indirectly required | Inhibits |
| Anemia type | Megaloblastic | Megaloblastic | Drug induced |
| Neurological symptoms | No | Yes | No |
| Therapeutic use | Supplementation | Supplementation | Anticancer, autoimmune |
Explanation:
Folate and vitamin B12 are closely linked in one carbon metabolism. Both deficiencies cause megaloblastic anemia. However, neurological deficits occur only in vitamin B12 deficiency. Methotrexate acts as an antifolate drug by inhibiting DHFR, thereby preventing THF formation and blocking DNA synthesis.
MCQs
- Folate is essential for synthesis of:
a) RNA only
b) DNA only
c) Proteins
d) Lipids
Answer: b) DNA only
- The active form of folate is:
a) Folic acid
b) Dihydrofolate
c) Tetrahydrofolate
d) Methionine
Answer: c) Tetrahydrofolate
- Folate is required for conversion of:
a) dTMP to dUMP
b) dUMP to dTMP
c) ATP to ADP
d) Homocysteine to cysteine
Answer: b) dUMP to dTMP
- Enzyme inhibited by methotrexate:
a) Thymidylate synthase
b) Dihydrofolate reductase
c) Methionine synthase
d) RNA polymerase
Answer: b) Dihydrofolate reductase
- Folate deficiency leads to:
a) Microcytic anemia
b) Hemolytic anemia
c) Megaloblastic anemia
d) Aplastic anemia
Answer: c) Megaloblastic anemia
- Folate is absorbed mainly in:
a) Duodenum
b) Jejunum
c) Ileum
d) Colon
Answer: b) Jejunum
- Folate participates in synthesis of:
a) Purines
b) Pyrimidines
c) Both
d) Neither
Answer: c) Both
- Neurological deficits are typical of:
a) Folate deficiency
b) Vitamin B12 deficiency
c) Iron deficiency
d) Vitamin C deficiency
Answer: b) Vitamin B12 deficiency
- Drug that inhibits bacterial DHFR:
a) Penicillin
b) Trimethoprim
c) Isoniazid
d) Rifampicin
Answer: b) Trimethoprim
- Excess folate may mask deficiency of:
a) Iron
b) Vitamin D
c) Vitamin B12
d) Vitamin A
Answer: c) Vitamin B12
FAQs
- Why does folate deficiency cause megaloblastic anemia?
Because impaired DNA synthesis delays nuclear maturation while cytoplasmic development continues. - Is folate safe in pregnancy?
Yes, it is essential to prevent neural tube defects. - Can folate correct neurological symptoms of B12 deficiency?
No, it may improve anemia but not neurological damage. - How does methotrexate relate to folate?
Methotrexate inhibits DHFR, blocking formation of active tetrahydrofolate. - How long does it take for folate stores to deplete?
Approximately 3 to 4 months. - What lab finding is seen in folate deficiency?
Elevated homocysteine with normal methylmalonic acid.
References
Goodman & Gilman’s Pharmacological Basis of Therapeutics
https://accessmedicine.mhmedical.com/book.aspx?bookID=2189
Katzung BG. Basic and Clinical Pharmacology
https://accessmedicine.mhmedical.com/book.aspx?bookID=2249
Tripathi KD. Essentials of Medical Pharmacology
https://jaypeedigital.com/book/9789354651970
Harrison’s Principles of Internal Medicine
https://accessmedicine.mhmedical.com/book.aspx?bookID=3095


