Table of Contents
Introduction
Furosemide, also known by its brand name Lasix, is a potent loop diuretic widely used in clinical practice to manage edema and hypertension. It acts quickly and effectively, making it a drug of choice in emergency settings like acute pulmonary edema or congestive heart failure (CHF).
It is a cornerstone medication in:
- Congestive heart failure
- Acute pulmonary edema
- Chronic kidney disease with volume overload
- Hypertension (especially with volume excess)
- Hypercalcemia (off-label)
Furosemide’s rapid onset, short duration, and high efficacy make it a must-know drug for medical, pharmacy, and nursing students in the U.S. preparing for exams such as USMLE Step 1, NCLEX-RN, NAPLEX, and PharmD coursework.
Stepwise Mechanism of Action of Furosemide
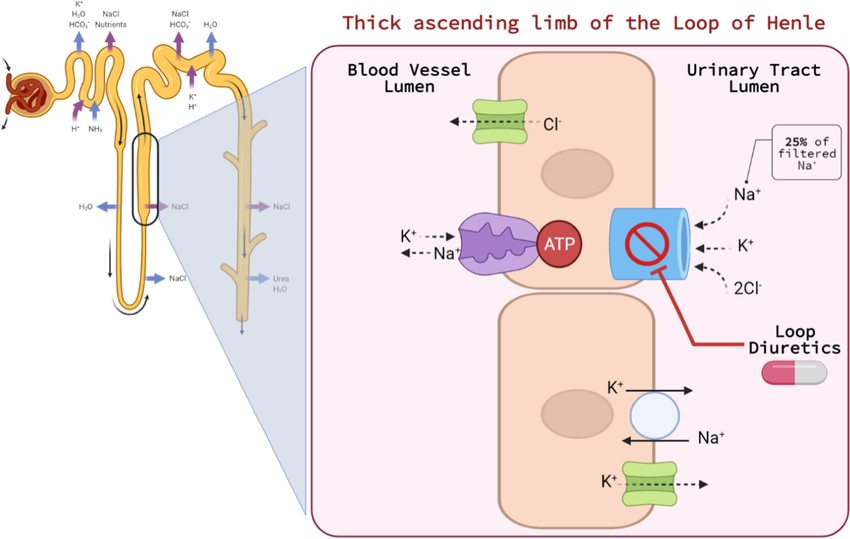
- Site of Action – Thick Ascending Limb (TAL):
Furosemide acts primarily on the thick ascending limb of the loop of Henle in the nephron. - Inhibition of Na⁺/K⁺/2Cl⁻ Cotransporter (NKCC2):
It selectively inhibits the NKCC2 symporter, blocking the reabsorption of sodium (Na⁺), potassium (K⁺), and chloride (Cl⁻) ions from the tubular lumen into the renal interstitium. - Disruption of Medullary Osmotic Gradient:
This decreases the concentration gradient necessary for water reabsorption in the collecting duct, resulting in increased urinary excretion of water (diuresis). - Increased Excretion of Other Ions:
Furosemide also promotes the loss of calcium (Ca²⁺), magnesium (Mg²⁺), potassium (K⁺), and hydrogen ions (H⁺), which can lead to electrolyte disturbances. - Rapid and Potent Diuresis:
Due to its high efficacy and rapid onset, it is especially useful in acute settings involving fluid overload or edema.
Pharmacokinetic Parameters of Furosemide
| Parameter | Value |
|---|---|
| Bioavailability | ~50% (oral); varies between individuals |
| Onset of Action | Oral: 30–60 minutes; IV: within 5 minutes |
| Half-life | ~1.5–2 hours |
| Protein Binding | ~95% |
| Metabolism | Partial hepatic metabolism |
| Excretion | Primarily renal (as unchanged drug) |
Clinical Uses of Furosemide
- Acute pulmonary edema
- Congestive heart failure (CHF)
- Nephrotic syndrome
- Chronic kidney disease (CKD) with fluid retention
- Liver cirrhosis with ascites
- Severe hypertension with fluid overload
- Hypercalcemia (off-label)
- Hyperkalemia (with saline and glucose)
Adverse Effects of Furosemide
- Hypokalemia
- Hyponatremia
- Hypocalcemia and hypomagnesemia
- Ototoxicity (dose-dependent, especially with IV use)
- Hyperuricemia (may trigger gout)
- Volume depletion and hypotension
- Allergic reactions (especially in sulfa-sensitive patients)
Comparative Analysis: Furosemide vs Hydrochlorothiazide
| Feature | Furosemide (Loop Diuretic) | Hydrochlorothiazide (Thiazide) |
|---|---|---|
| Site of Action | Thick ascending limb (NKCC2) | Distal convoluted tubule (NCC) |
| Efficacy | High (strong natriuresis) | Moderate |
| Onset of Action | Fast (IV: 5 mins, oral: 30–60 mins) | Slower (2–4 hours) |
| Use in CKD | Preferred | Less effective at low GFR |
| Calcium Excretion | Increases (hypocalcemia) | Decreases (hypercalcemia) |
| Electrolyte Loss | More pronounced | Moderate |
Practice MCQs
Q1. Furosemide acts on which part of the nephron?
A. Proximal tubule
B. Distal tubule
C. Thick ascending limb ✅
D. Collecting duct
Q2. The primary transporter inhibited by furosemide is:
A. Na⁺/Cl⁻ symporter
B. ENaC
C. Na⁺/K⁺/2Cl⁻ cotransporter ✅
D. H⁺/K⁺ ATPase
Q3. Which electrolyte disturbance is most associated with furosemide use?
A. Hyperkalemia
B. Hypokalemia ✅
C. Hypernatremia
D. Hypercalcemia
Q4. What is the onset of action for intravenous furosemide?
A. 30 minutes
B. 1 hour
C. 5 minutes ✅
D. 2 hours
Q5. Furosemide is used in all of the following EXCEPT:
A. Pulmonary edema
B. Liver cirrhosis
C. Diabetes insipidus ✅
D. Heart failure
Q6. A rare but serious side effect of furosemide is:
A. Retinopathy
B. Ototoxicity ✅
C. Hepatitis
D. Asthma
Q7. Which drug should be used cautiously with furosemide to avoid excessive ototoxicity?
A. Digoxin
B. Metformin
C. Aminoglycosides ✅
D. Statins
Q8. Furosemide may increase the risk of:
A. Hypouricemia
B. Hyperuricemia ✅
C. Hyperglycemia
D. Hypophosphatemia
Q9. In patients with sulfonamide allergy, furosemide may cause:
A. Cardiac arrhythmias
B. Hemolytic anemia
C. Hypersensitivity reaction ✅
D. Stevens-Johnson syndrome
Q10. Which of the following is TRUE regarding furosemide?
A. It decreases calcium excretion
B. It has a long half-life
C. It is effective at low GFR ✅
D. It reduces LDL cholesterol
FAQs
Q1: Can furosemide be used in patients with kidney failure?
Yes, it is effective in patients with low GFR and is preferred over thiazides in CKD.
Q2: Does furosemide cause ototoxicity?
Yes, especially at high doses or when given rapidly IV. Risk increases when combined with aminoglycosides.
Q3: Should potassium supplements be used with furosemide?
Yes, they are often co-prescribed to prevent hypokalemia.
Q4: Is furosemide safe in pregnancy?
It should only be used if clearly needed; monitor fluid and electrolyte balance carefully.
References
- KD Tripathi – Essentials of Medical Pharmacology
- Goodman & Gilman – The Pharmacological Basis of Therapeutics
- Review of Pharmacology – Sparsh Gupta


