
Table of Contents
Introduction
Teriparatide is a recombinant form of the first 34 amino acids of human parathyroid hormone (PTH 1-34), which represents the biologically active portion of the hormone. It is used primarily as an anabolic agent in the treatment of osteoporosis. Teriparatide is unique among osteoporosis therapies because it stimulates new bone formation rather than merely inhibiting bone resorption.


Mechanism of Action (Step-wise)
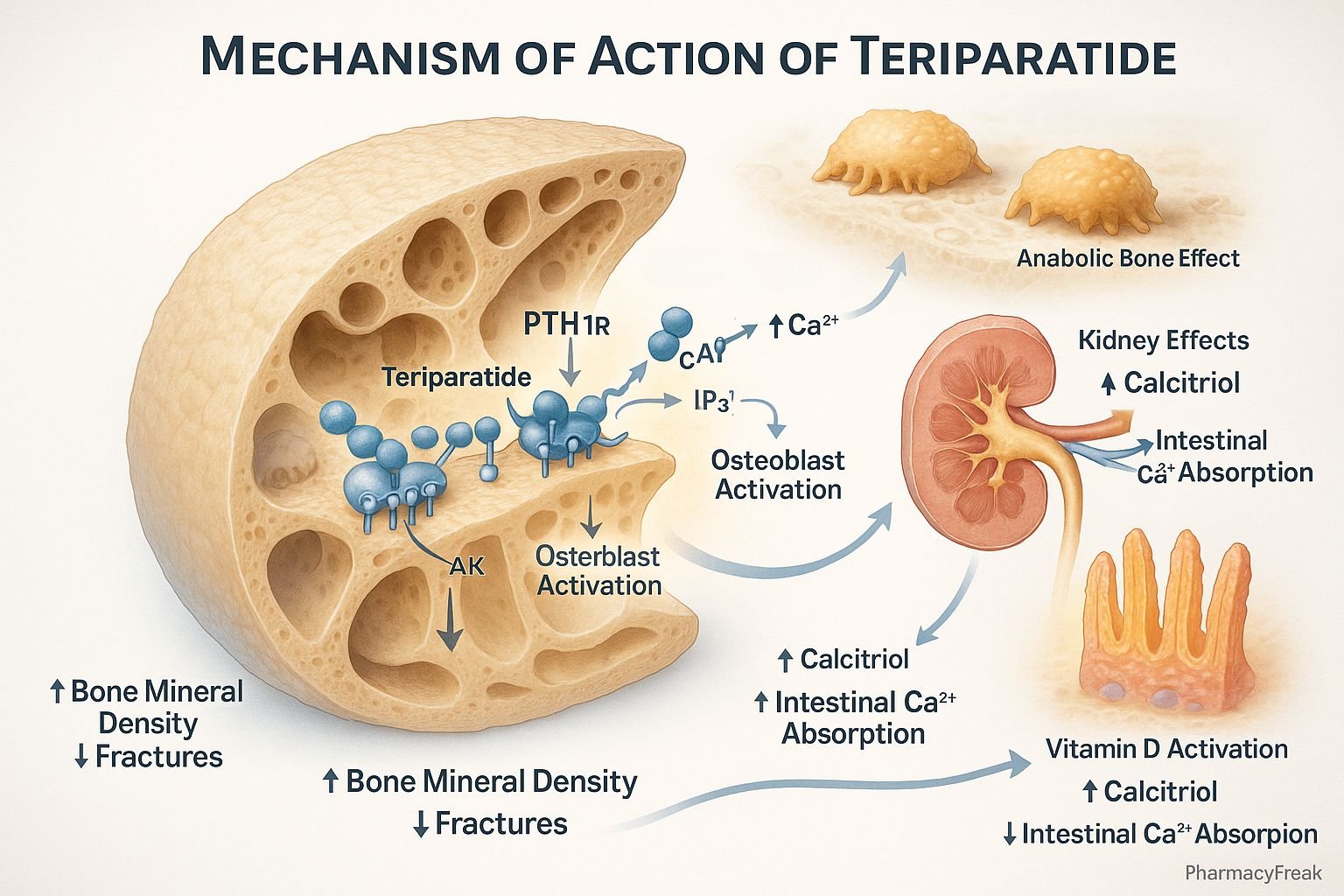
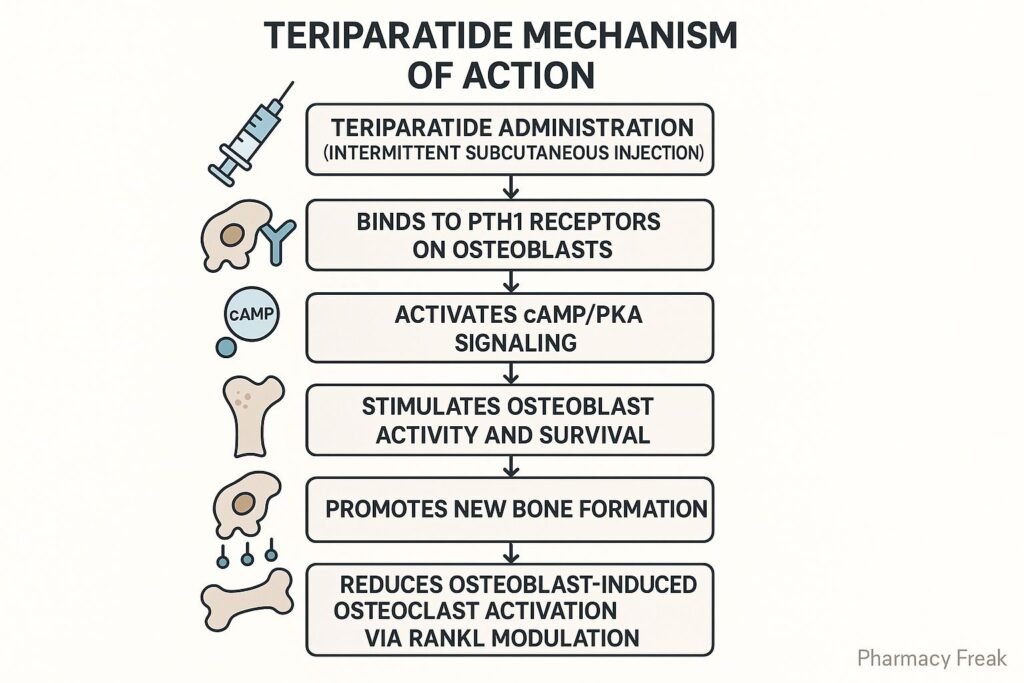
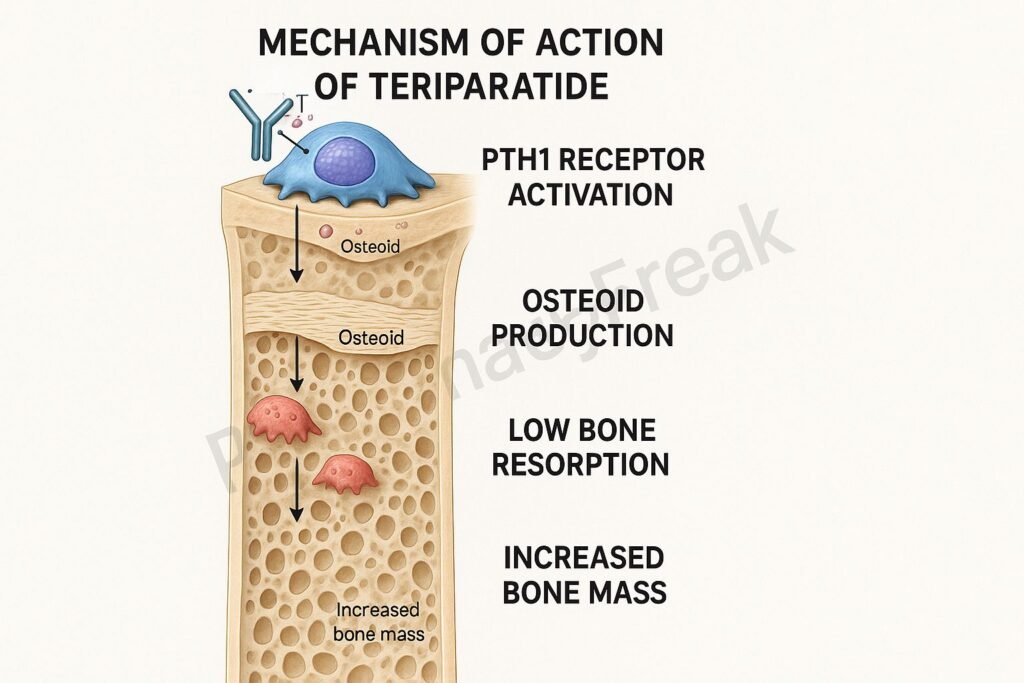
1. Binding to PTH Receptors (PTH1R)
Teriparatide binds to the PTH1 receptor, which is predominantly expressed on osteoblasts and osteoblast precursors.
2. Activation of Adenylyl Cyclase Pathway
The receptor activation stimulates the Gs protein–coupled pathway, leading to activation of adenylyl cyclase and an increase in cyclic AMP (cAMP).
3. Protein Kinase A Activation
cAMP activates protein kinase A (PKA), which initiates gene transcription leading to osteoblast differentiation and activity.
4. Promotion of Osteoblast Survival
Teriparatide promotes survival of mature osteoblasts and reduces apoptosis, enhancing bone formation.
5. Intermittent Dosing Effect
Intermittent (once-daily) administration favors anabolic activity (bone formation), whereas continuous exposure leads to bone resorption.
6. Net Increase in Bone Mass
The cumulative effect of increased osteoblastic activity results in improved bone mass and strength.
Pharmacokinetics
- Route of Administration: Subcutaneous injection
- Bioavailability: ~95%
- Onset of Action: Rapid absorption; peak levels within 30 minutes
- Half-Life: ~1 hour
- Metabolism: Hepatic and extrahepatic degradation
- Excretion: Primarily renal as inactive metabolites
Clinical Uses
- Postmenopausal osteoporosis in women at high fracture risk
- Primary or hypogonadal osteoporosis in men at high fracture risk
- Glucocorticoid-induced osteoporosis
Note: Treatment duration is typically limited to 2 years due to risk of osteosarcoma observed in animal studies.
Adverse Effects
- Common: Nausea, leg cramps, dizziness, hypercalcemia
- Serious: Hypercalciuria, orthostatic hypotension post-injection
- Contraindications:
- Paget’s disease
- Unexplained elevations in alkaline phosphatase
- Prior skeletal radiation therapy
- Bone metastases or history of skeletal malignancy
Comparative Analysis
| Parameter | Teriparatide | Alendronate |
|---|---|---|
| Drug Class | PTH analog | Bisphosphonate |
| Mechanism | Stimulates bone formation | Inhibits bone resorption |
| Dosing Frequency | Daily injection | Weekly oral |
| Effect on Bone Remodeling | Anabolic | Antiresorptive |
| Max Duration of Use | 2 years | Indefinite |
| Risk of Osteosarcoma | Yes (in animals) | No |
Multiple Choice Questions (MCQs)
1. Teriparatide is a synthetic analog of which hormone?
a) Calcitonin
b) Vitamin D
c) Parathyroid hormone
d) Estrogen
Answer: c) Parathyroid hormone
2. How does teriparatide affect bone?
a) Inhibits osteoblasts
b) Stimulates bone resorption
c) Increases bone formation
d) Suppresses calcium absorption
Answer: c) Increases bone formation
3. Which receptor does teriparatide primarily act on?
a) Calcitonin receptor
b) Estrogen receptor
c) Vitamin D receptor
d) PTH1 receptor
Answer: d) PTH1 receptor
4. What is the typical route of administration for teriparatide?
a) Oral
b) Intramuscular
c) Intravenous
d) Subcutaneous
Answer: d) Subcutaneous
5. Why is teriparatide therapy duration limited?
a) Causes hypocalcemia
b) Risk of osteosarcoma
c) Induces vitamin D deficiency
d) Increases phosphate levels
Answer: b) Risk of osteosarcoma
FAQs
Q1. Can teriparatide be used in men with osteoporosis?
Yes, it is indicated for men with primary or hypogonadal osteoporosis at high fracture risk.
Q2. Is daily administration of teriparatide important?
Yes, intermittent daily dosing promotes bone formation, unlike continuous exposure.
Q3. What calcium-related side effects are seen with teriparatide?
Hypercalcemia and hypercalciuria may occur; serum calcium levels should be monitored.
Q4. Can teriparatide be combined with bisphosphonates?
It is not typically recommended to use concurrently as their mechanisms differ and may counteract.
Q5. Is teriparatide safe during pregnancy?
No, it is contraindicated in pregnancy due to lack of safety data.
References
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics, 12th Edition
- KD Tripathi, Essentials of Medical Pharmacology, 7th Edition
- Prescribing information for teriparatide
- Clinical practice guidelines on osteoporosis management


