Table of Contents
Introduction
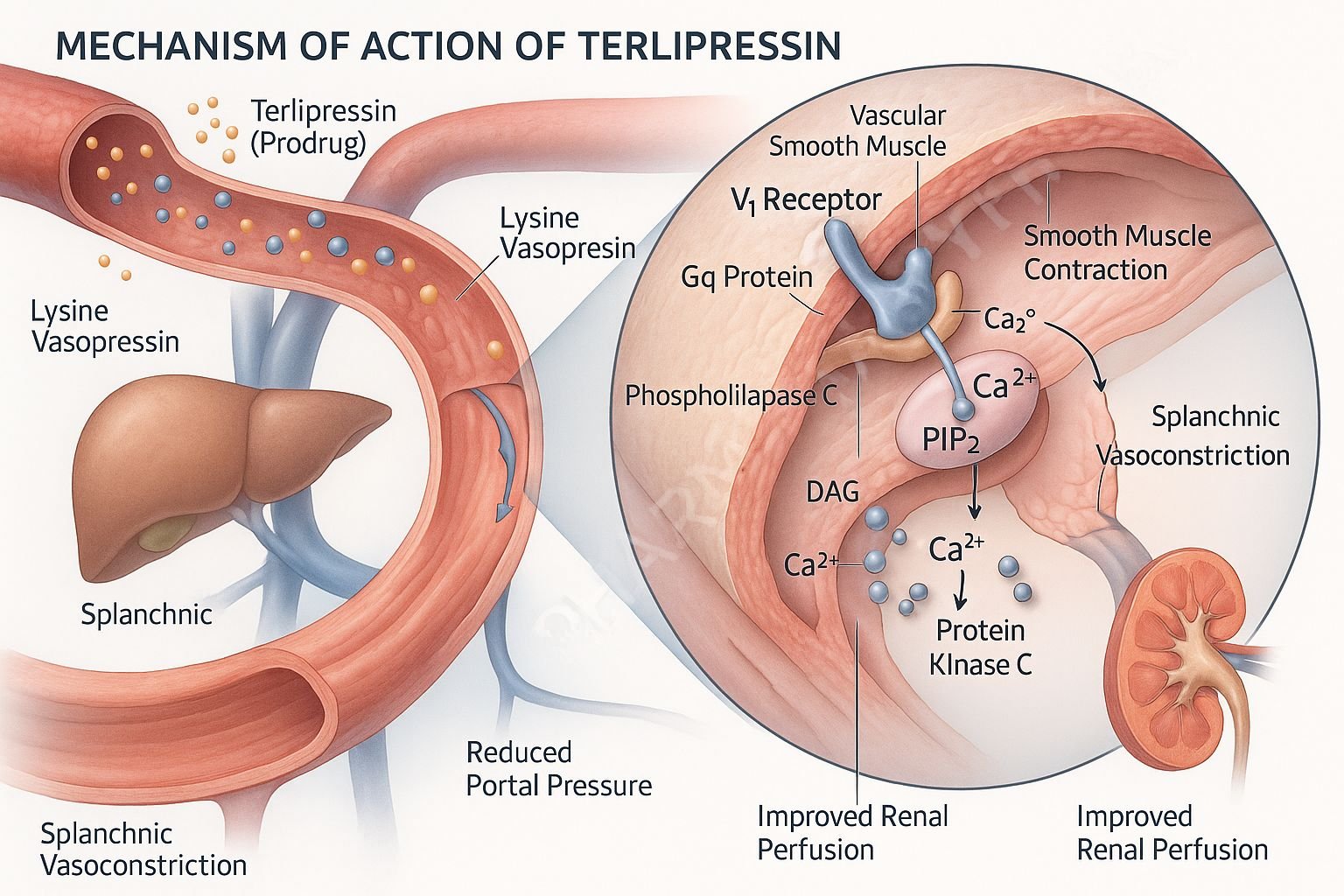
Terlipressin is a synthetic vasopressin analogue and prodrug of lysine-vasopressin, primarily used to manage acute variceal bleeding and hepatorenal syndrome (HRS) in patients with advanced liver disease. It exerts selective vasoconstrictive effects through vasopressin V1 receptors, targeting the splanchnic circulation to improve effective arterial blood volume and renal perfusion.

Mechanism of Action (Step-wise)
1. Prodrug Conversion to Lysine‑Vasopressin
Terlipressin is enzymatically cleaved by tissue peptidases to release its active form, lysine‑vasopressin (L‑VP), which possesses full V1 and V2 receptor agonist activity.
2. V1 Receptor Activation (Gq‑coupled)
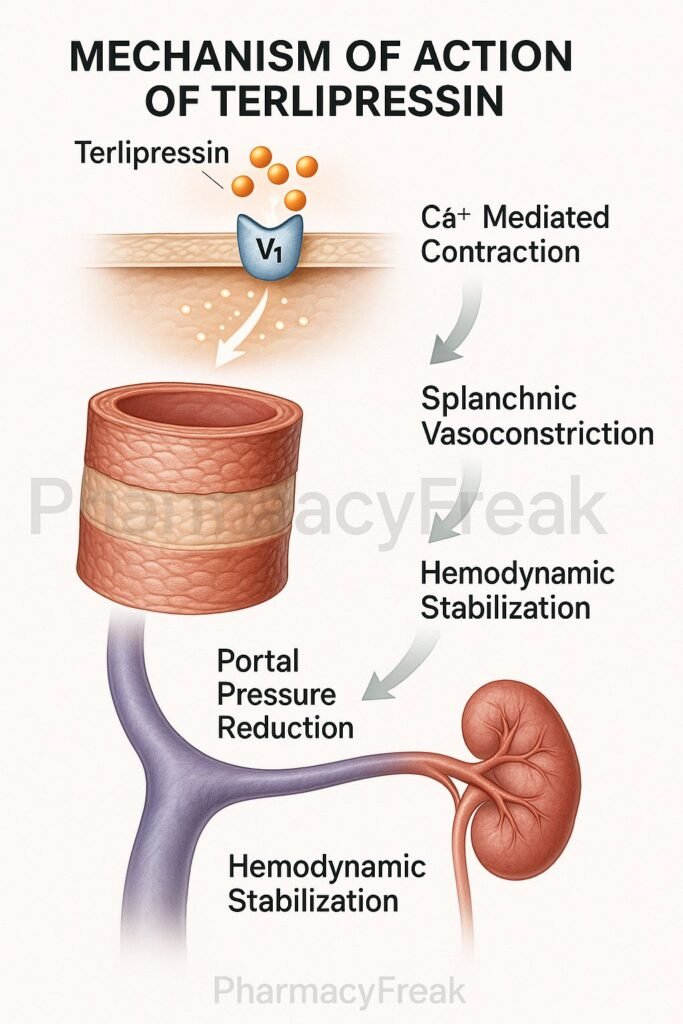
Activation of V1 receptors on vascular smooth muscle increases intracellular calcium, leading to potent vasoconstriction—particularly in the splanchnic and systemic circulations.
3. Reduced Portal Pressure and Improved Circulating Volume
Splanchnic vasoconstriction reduces portal venous pressure and redistributes blood to systemic circulation, improving mean arterial pressure (MAP) and enhancing renal blood flow.
4. Minimal Antidiuretic (V2) Effect
While L‑VP can activate V2 receptors, its antidiuretic action is clinically minimal compared to vasopressin.
5. Sustained Action via Active Metabolite Release
Terlipressin’s slow and sustained conversion to L‑VP accounts for its longer duration of vasoconstrictive effect (approximately 4–6 hours) compared to native vasopressin.
Pharmacokinetics
- Administration & Metabolism: Administered intravenously; rapidly metabolized by peptidases into L‑VP.
- Half‑Life: Terlipressin’s terminal half-life is approximately 0.9 hours; L‑VP’s is around 3 hours.
- Clearance & Volume of Distribution: Terlipressin clearance is approximately 27.4 L/h; L‑VP clearance is approximately 318 L/h. Volume of distribution: terlipressin ≈ 6 L; L‑VP ≈ 1370 L.
Clinical Uses
- Acute Variceal Bleeding: Helps control hemorrhage by reducing portal pressure.
- Hepatorenal Syndrome (HRS): Improves renal function by restoring MAP and reducing vasodilation.
- Occasional Use in Septic Shock: Especially in catecholamine-resistant cases.
Adverse Effects & Precautions
- Risks of Ischemia: Excessive vasoconstriction may worsen myocardial, peripheral, or mesenteric ischemia.
- Respiratory Compromise: Contraindicated in hypoxic patients; monitor oxygenation closely.
- Cardiovascular Effects: May cause arrhythmias, elevated blood pressure, or reduced cardiac output.
Comparative Analysis
| Feature | Terlipressin | Vasopressin |
|---|---|---|
| Prodrug Activity | Yes (to L‑VP) | No |
| V1 Receptor Selectivity | Higher | Balanced V1 & V2 |
| Duration of Action | Longer (4–6 hours) | Shorter |
| Clinical Use | Variceal bleed, HRS | Broader vasoactive applications |
| Antidiuretic Effect | Minimal | Stronger (via V2) |
Multiple Choice Questions (MCQs)
1. Terlipressin is primarily a prodrug for which molecule?
a) Cortisol
b) Lysine‑vasopressin
c) Norepinephrine
d) Aldosterone
Answer: b) Lysine‑vasopressin
2. Which receptor mediates the vasoconstrictive action of terlipressin?
a) V1 receptor
b) V2 receptor
c) Beta‑adrenergic receptor
d) Muscarinic receptor
Answer: a) V1 receptor
3. What is the main therapeutic benefit of terlipressin in hepatorenal syndrome?
a) Increased portal pressure
b) Enhanced renal perfusion
c) Reduced arterial pressure
d) Diuretic effect
Answer: b) Enhanced renal perfusion
4. The duration of terlipressin’s effect is prolonged due to which factor?
a) High potency of parent drug
b) Slow release of active metabolite L‑VP
c) Long half-life of terlipressin
d) Lipid solubility
Answer: b) Slow release of active metabolite L‑VP
5. One serious adverse effect of terlipressin is:
a) Hypoglycemia
b) Ischemia in vital organs
c) Hypernatremia
d) CNS depression
Answer: b) Ischemia in vital organs
FAQs
Q1. Why is terlipressin preferred over vasopressin in some cases?
Its prodrug formulation allows longer-lasting V1-mediated vasoconstriction with fewer dosing intervals.
Q2. Can terlipressin be used in septic shock?
Use is limited; some clinical settings may use it in norepinephrine-resistant cases under careful monitoring.
Q3. Why is terlipressin contraindicated in hypoxic patients?
Because worsening vasoconstriction may impair oxygen delivery to already compromised tissues.
References
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics, 12th Edition
- KD Tripathi, Essentials of Medical Pharmacology, 7th Edition
- Clinical literature on hepatorenal syndrome treatment
- Terlipressin FDA monograph and drug label
- Comparative studies of vasopressin analogues

