
Table of Contents
Introduction
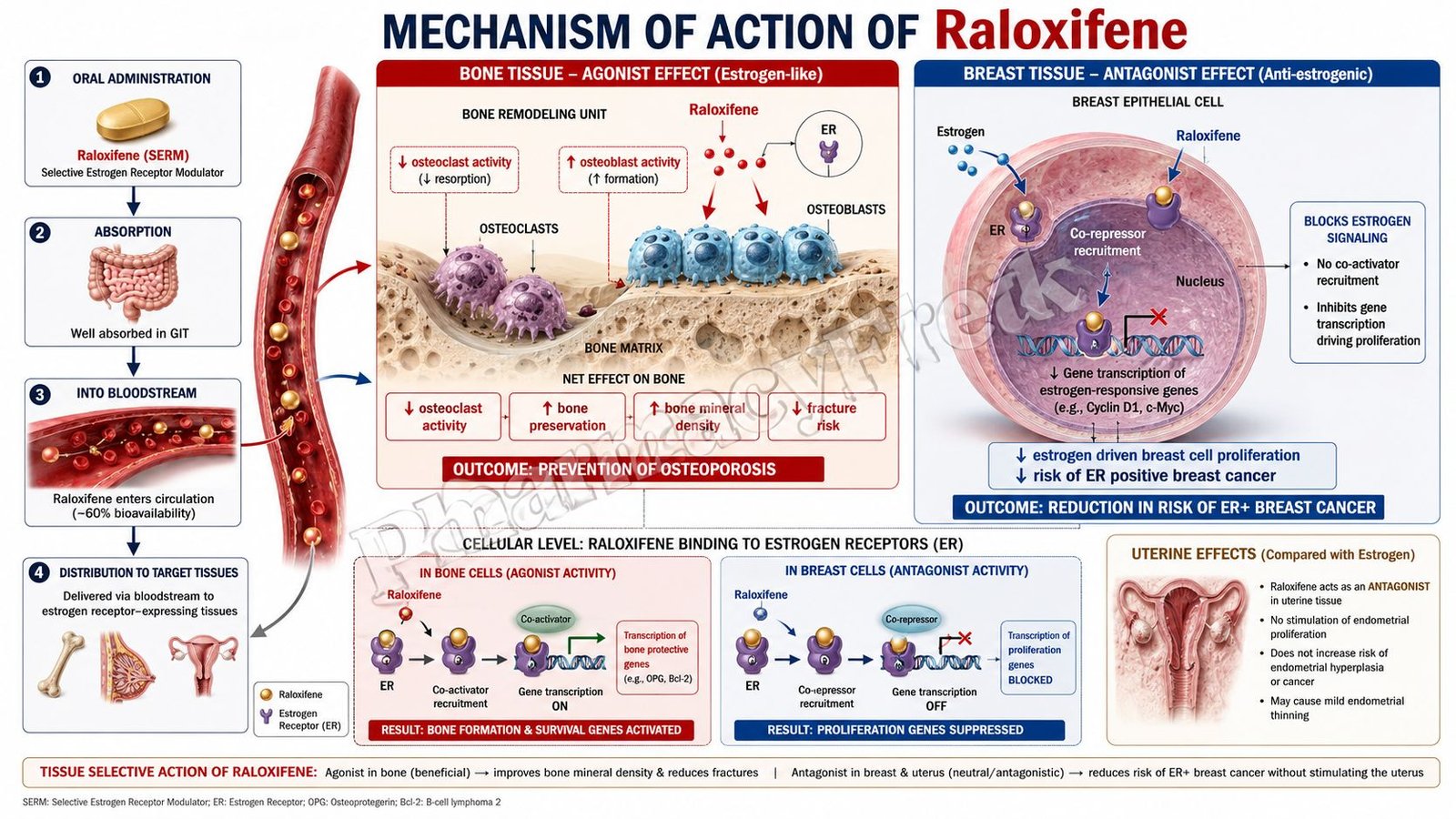
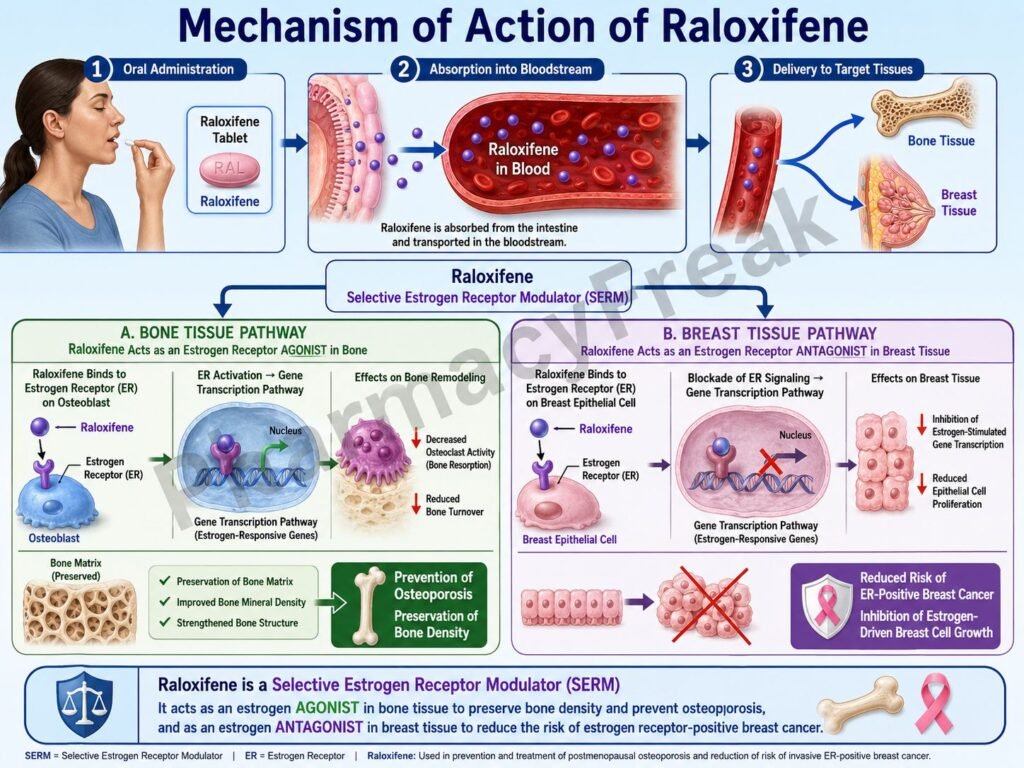
Raloxifene is a selective estrogen receptor modulator (SERM) used primarily in the prevention and treatment of osteoporosis in postmenopausal women. It exhibits estrogen agonist effects on bone and lipid metabolism while acting as an estrogen antagonist in breast and uterine tissue. This tissue-selective activity allows raloxifene to provide beneficial skeletal effects with reduced risk of endometrial stimulation.
Mechanism of Action (Step-wise)
- Raloxifene binds selectively to estrogen receptors (ERs).
- It interacts mainly with nuclear estrogen receptors ERα and ERβ.
- After binding, the raloxifene-receptor complex translocates to the nucleus.
- The complex binds to estrogen response elements (EREs) on DNA.
- Gene transcription is altered in a tissue-specific manner.
- In bone tissue, raloxifene acts as an estrogen agonist.
- Estrogen receptor activation decreases osteoclast activity and bone resorption.
- Reduced bone resorption increases bone mineral density.
- In breast tissue, raloxifene acts as an estrogen antagonist.
- This reduces estrogen-mediated proliferation of breast tissue.
- In the uterus, raloxifene has minimal stimulatory activity.
- It also improves lipid profile by decreasing LDL cholesterol levels.
- The overall effect is preservation of bone mass with reduced estrogenic stimulation of breast and uterine tissues.
A key exam point is that raloxifene is a SERM with estrogen agonist effects on bone and antagonist effects on breast tissue.

Pharmacokinetics
Raloxifene is administered orally and undergoes extensive first-pass metabolism. It is highly protein bound and undergoes enterohepatic circulation, contributing to prolonged action. The drug is metabolized mainly in the liver through glucuronidation and excreted primarily in feces.
Clinical Uses
Raloxifene is used in prevention and treatment of postmenopausal osteoporosis. It is also used to reduce the risk of invasive breast cancer in postmenopausal women with osteoporosis or high breast cancer risk.
Adverse Effects
Common adverse effects include hot flashes, leg cramps, and peripheral edema. A major serious adverse effect is increased risk of venous thromboembolism. Unlike tamoxifen, raloxifene has minimal risk of endometrial hyperplasia or endometrial carcinoma.
Comparative Analysis
| Feature | Raloxifene | Tamoxifen | Estrogen Therapy |
|---|---|---|---|
| Drug class | SERM | SERM | Hormone replacement |
| Bone effect | Estrogen agonist | Partial agonist | Agonist |
| Breast tissue effect | Antagonist | Antagonist | Agonist |
| Uterine effect | Minimal stimulation | Partial agonist | Agonist |
| Osteoporosis use | Yes | Limited | Yes |
| Endometrial cancer risk | Minimal | Increased | Increased |
Raloxifene differs from tamoxifen because it has minimal estrogenic stimulation of the uterus. Compared with estrogen therapy, it provides bone protection without strong stimulation of breast and endometrial tissue.
MCQs
- Raloxifene belongs to which drug class?
a) Aromatase inhibitors
b) Selective estrogen receptor modulators
c) Bisphosphonates
d) Progestins
Answer: b) Selective estrogen receptor modulators
- Raloxifene acts as an estrogen agonist mainly in:
a) Breast tissue
b) Bone tissue
c) Uterine tissue only
d) Prostate tissue
Answer: b) Bone tissue
- Raloxifene reduces activity of:
a) Osteoblasts
b) Osteoclasts
c) Fibroblasts
d) Chondrocytes
Answer: b) Osteoclasts
- Raloxifene is mainly used in:
a) Hyperthyroidism
b) Postmenopausal osteoporosis
c) Asthma
d) Diabetes mellitus
Answer: b) Postmenopausal osteoporosis
- In breast tissue, raloxifene acts as a:
a) Full agonist
b) Antagonist
c) Enzyme activator
d) Histamine blocker
Answer: b) Antagonist
- Raloxifene decreases risk of:
a) Invasive breast cancer
b) Hyperthyroidism
c) Peptic ulcer disease
d) Migraine
Answer: a) Invasive breast cancer
- A major adverse effect is:
a) Hypoglycemia
b) Venous thromboembolism
c) Hypercalcemia
d) Bradycardia
Answer: b) Venous thromboembolism
- Compared with tamoxifen, raloxifene has lower risk of:
a) Osteoporosis
b) Endometrial carcinoma
c) Hot flashes
d) Leg cramps
Answer: b) Endometrial carcinoma
- Raloxifene binds to:
a) Dopamine receptors
b) Estrogen receptors
c) Histamine receptors
d) Muscarinic receptors
Answer: b) Estrogen receptors
- Raloxifene improves lipid profile by reducing:
a) HDL cholesterol
b) LDL cholesterol
c) Triglyceride synthesis only
d) Calcium absorption
Answer: b) LDL cholesterol
- Raloxifene undergoes significant:
a) Renal activation
b) First-pass metabolism
c) Pulmonary metabolism
d) Skin metabolism
Answer: b) First-pass metabolism
- Compared with estrogen therapy, raloxifene has:
a) Greater uterine stimulation
b) Less endometrial stimulation
c) No effect on bone
d) Greater breast stimulation
Answer: b) Less endometrial stimulation
FAQs
What is the mechanism of action of raloxifene?
Raloxifene selectively modulates estrogen receptors, acting as an agonist in bone and antagonist in breast tissue.
Why is raloxifene used in osteoporosis?
Because it reduces bone resorption and increases bone mineral density.
How does raloxifene reduce breast cancer risk?
By blocking estrogen-mediated proliferation in breast tissue.
Does raloxifene stimulate the uterus?
It has minimal uterine stimulation compared with tamoxifen or estrogen therapy.
What is a major serious adverse effect?
Venous thromboembolism.
Is raloxifene considered hormone replacement therapy?
No, it is a selective estrogen receptor modulator.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics – Estrogens and Selective Estrogen Receptor Modulators
https://accessmedicine.mhmedical.com/book.aspx?bookid=3191
Katzung: Basic and Clinical Pharmacology – Estrogens and Antiestrogens
https://accessmedicine.mhmedical.com/content.aspx?bookid=3382
Tripathi: Essentials of Medical Pharmacology – Hormones and Antihormones
https://www.jaypeedigital.com
Harrison’s Principles of Internal Medicine – Osteoporosis and Menopause
https://accessmedicine.mhmedical.com

