Table of Contents
Introduction
General anesthesia is a reversible drug induced state characterized by unconsciousness, amnesia, analgesia, and immobility with suppression of autonomic responses. It is produced by a combination of intravenous and inhalational anesthetic agents acting on the central nervous system. Unlike a single drug mechanism, general anesthesia represents a coordinated depression of neuronal activity across cortical, thalamic, spinal, and brainstem networks.
The molecular basis involves modulation of inhibitory and excitatory neurotransmission, primarily through gamma aminobutyric acid (GABA), N methyl D aspartate (NMDA), glycine, and two pore domain potassium channels. Understanding its mechanism is essential for USMLE, NEET PG, FMGE, PLAB, INICET, NCLEX, and MCCQE.

Mechanism of Action (Step-wise)
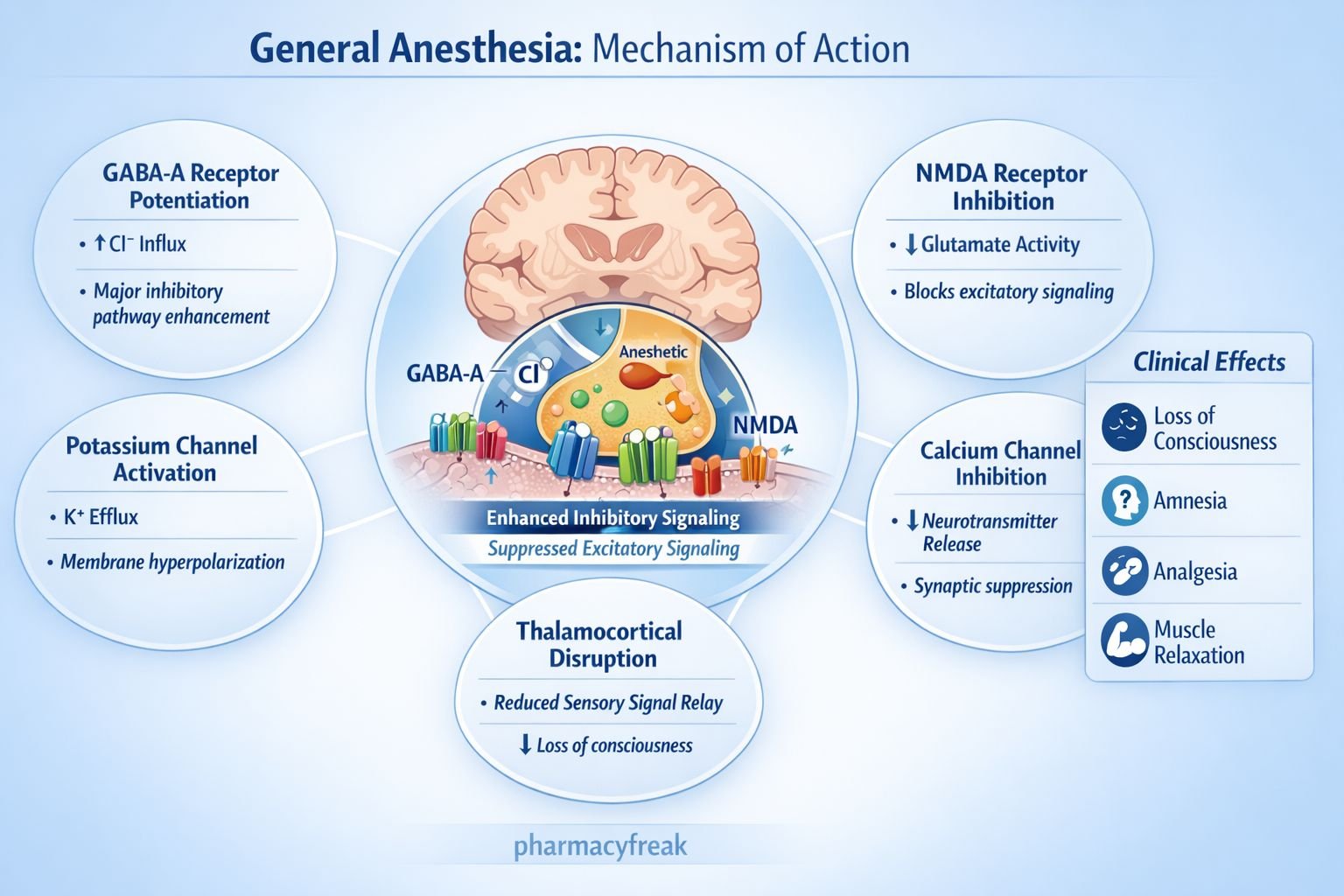
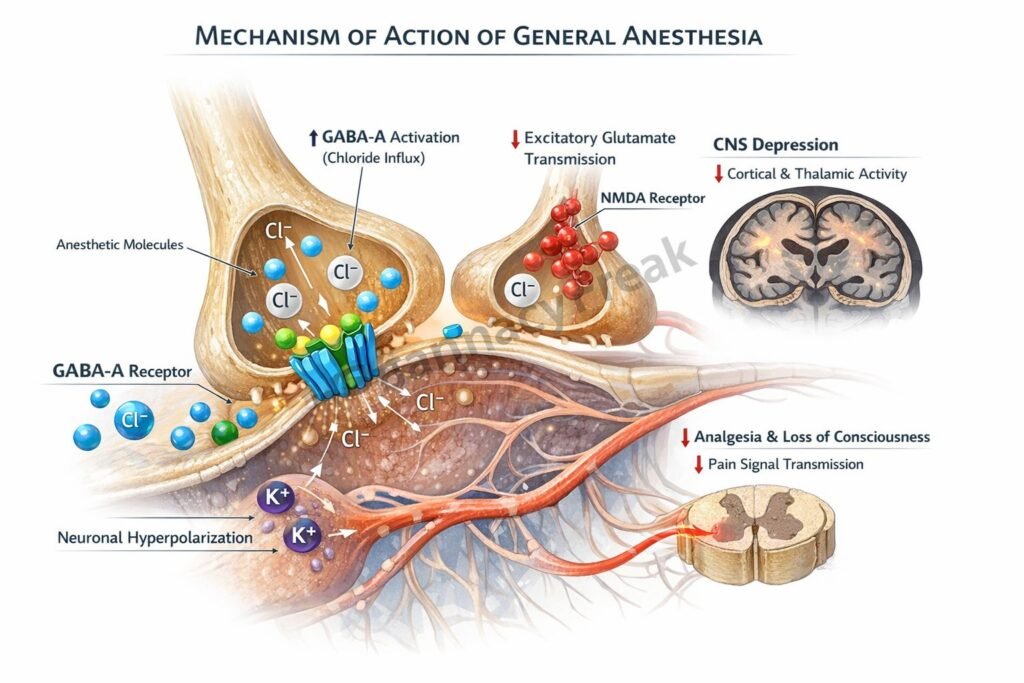
General anesthetics act at multiple CNS sites to produce unconsciousness and immobility.
Step 1: Enhancement of inhibitory neurotransmission
Many intravenous agents such as propofol and thiopental enhance GABA A receptor activity, increasing chloride influx and causing neuronal hyperpolarization.
Step 2: Inhibition of excitatory transmission
Agents such as ketamine and nitrous oxide inhibit NMDA receptors, reducing glutamate mediated excitatory signaling.
Step 3: Activation of potassium channels
Volatile anesthetics activate two pore domain potassium channels, increasing potassium efflux and stabilizing hyperpolarized neuronal membranes.
Step 4: Spinal cord depression
Immobility in response to painful stimuli is mainly due to suppression of spinal motor reflex pathways.
Step 5: Thalamocortical disruption
Anesthetics disrupt thalamocortical connectivity, preventing sensory information processing and producing unconsciousness.
Overall effect:
Global CNS depression leading to loss of consciousness, analgesia, amnesia, and muscle relaxation.
Key exam concept:
Immobility correlates strongly with spinal cord suppression, whereas unconsciousness correlates with cortical and thalamic effects.
Pharmacokinetics
Intravenous anesthetics:
- Rapid onset due to high lipid solubility
- Redistribution from brain to muscle and fat determines duration
- Hepatic metabolism and renal excretion
Inhalational anesthetics:
- Absorbed via alveoli
- Onset determined by blood gas partition coefficient
- Eliminated primarily via lungs
Minimum alveolar concentration (MAC):
- Measure of anesthetic potency
- Lower MAC indicates higher potency
Clinical Uses
- Induction and maintenance of surgical anesthesia
- Procedural sedation
- Intensive care unit sedation
- Electroconvulsive therapy
- Facilitation of mechanical ventilation
Balanced anesthesia often combines:
- Intravenous induction agent
- Inhalational maintenance agent
- Opioid analgesic
- Neuromuscular blocker
Adverse Effects
Common adverse effects:
- Hypotension due to vasodilation
- Respiratory depression
- Postoperative nausea and vomiting
Serious adverse effects:
- Malignant hyperthermia with volatile anesthetics and succinylcholine
- Increased intracranial pressure with some agents
- Emergence delirium
Organ specific risks:
- Hepatotoxicity with halothane
- Nephrotoxicity with older agents
Comparative Analysis
| Feature | Propofol | Ketamine | Isoflurane |
|---|---|---|---|
| Primary receptor | GABA A | NMDA antagonist | GABA modulation + K channel |
| Analgesia | Minimal | Strong | Moderate |
| Hemodynamics | Hypotension | Increases BP | Vasodilation |
| Route | IV | IV | Inhalational |
| Emergence | Rapid | Delirium possible | Moderate |
Explanation:
Propofol primarily enhances GABA mediated inhibition, producing rapid unconsciousness but minimal analgesia. Ketamine blocks NMDA receptors and produces dissociative anesthesia with preserved airway reflexes and increased sympathetic tone. Isoflurane acts via multiple mechanisms including GABA potentiation and potassium channel activation, producing balanced anesthesia.
MCQs
- Most intravenous anesthetics act by enhancing:
a) Dopamine receptors
b) GABA A receptors
c) Serotonin receptors
d) Acetylcholine receptors
Answer: b) GABA A receptors
- Ketamine primarily blocks:
a) GABA A
b) NMDA
c) Glycine
d) Opioid receptors
Answer: b) NMDA
- Immobility during anesthesia is mainly mediated at the:
a) Cortex
b) Hippocampus
c) Spinal cord
d) Cerebellum
Answer: c) Spinal cord
- MAC is a measure of:
a) Solubility
b) Potency
c) Clearance
d) Toxicity
Answer: b) Potency
- Propofol commonly causes:
a) Hypertension
b) Hypotension
c) Tachycardia
d) Bronchospasm
Answer: b) Hypotension
- Malignant hyperthermia is associated with:
a) Ketamine
b) Propofol
c) Volatile anesthetics
d) Midazolam
Answer: c) Volatile anesthetics
- Rapid recovery from IV anesthetics is due to:
a) Renal clearance
b) Redistribution
c) Hepatic metabolism
d) Lung excretion
Answer: b) Redistribution
- Nitrous oxide acts mainly on:
a) Sodium channels
b) NMDA receptors
c) GABA receptors
d) Beta receptors
Answer: b) NMDA receptors
- Which agent increases blood pressure?
a) Propofol
b) Isoflurane
c) Ketamine
d) Thiopental
Answer: c) Ketamine
- Inhalational anesthetics are eliminated primarily via:
a) Kidney
b) Liver
c) Lungs
d) Bile
Answer: c) Lungs
FAQs
- How do general anesthetics cause unconsciousness?
By disrupting thalamocortical signaling and enhancing inhibitory neurotransmission. - Why is ketamine called dissociative anesthesia?
Because it produces functional dissociation between thalamus and limbic system. - What determines speed of inhalational induction?
Blood gas partition coefficient and ventilation rate. - Why is balanced anesthesia used?
To combine hypnosis, analgesia, and muscle relaxation while minimizing side effects. - What is MAC?
Minimum alveolar concentration required to prevent movement in 50 percent of patients. - Are all general anesthetics GABA agonists?
No. Some act via NMDA inhibition or potassium channel activation.
References
Goodman & Gilman’s Pharmacological Basis of Therapeutics
https://accessmedicine.mhmedical.com/book.aspx?bookID=2189
Katzung BG. Basic and Clinical Pharmacology
https://accessmedicine.mhmedical.com/book.aspx?bookID=2249
Tripathi KD. Essentials of Medical Pharmacology
https://jaypeedigital.com/book/9789354651970
Harrison’s Principles of Internal Medicine
https://accessmedicine.mhmedical.com/book.aspx?bookID=3095

