Table of Contents
Introduction
Fluoroquinolones are a broad-spectrum class of synthetic antibacterial agents widely used in the treatment of gram-negative, gram-positive, atypical, and intracellular bacterial infections. Common drugs in this class include ciprofloxacin, levofloxacin, moxifloxacin, and norfloxacin. Fluoroquinolones are extremely high-yield for pharmacology and clinical examinations due to their unique DNA-targeting mechanism, concentration-dependent killing, and characteristic musculoskeletal and CNS toxicities.
Mechanism of Action (Step-wise)
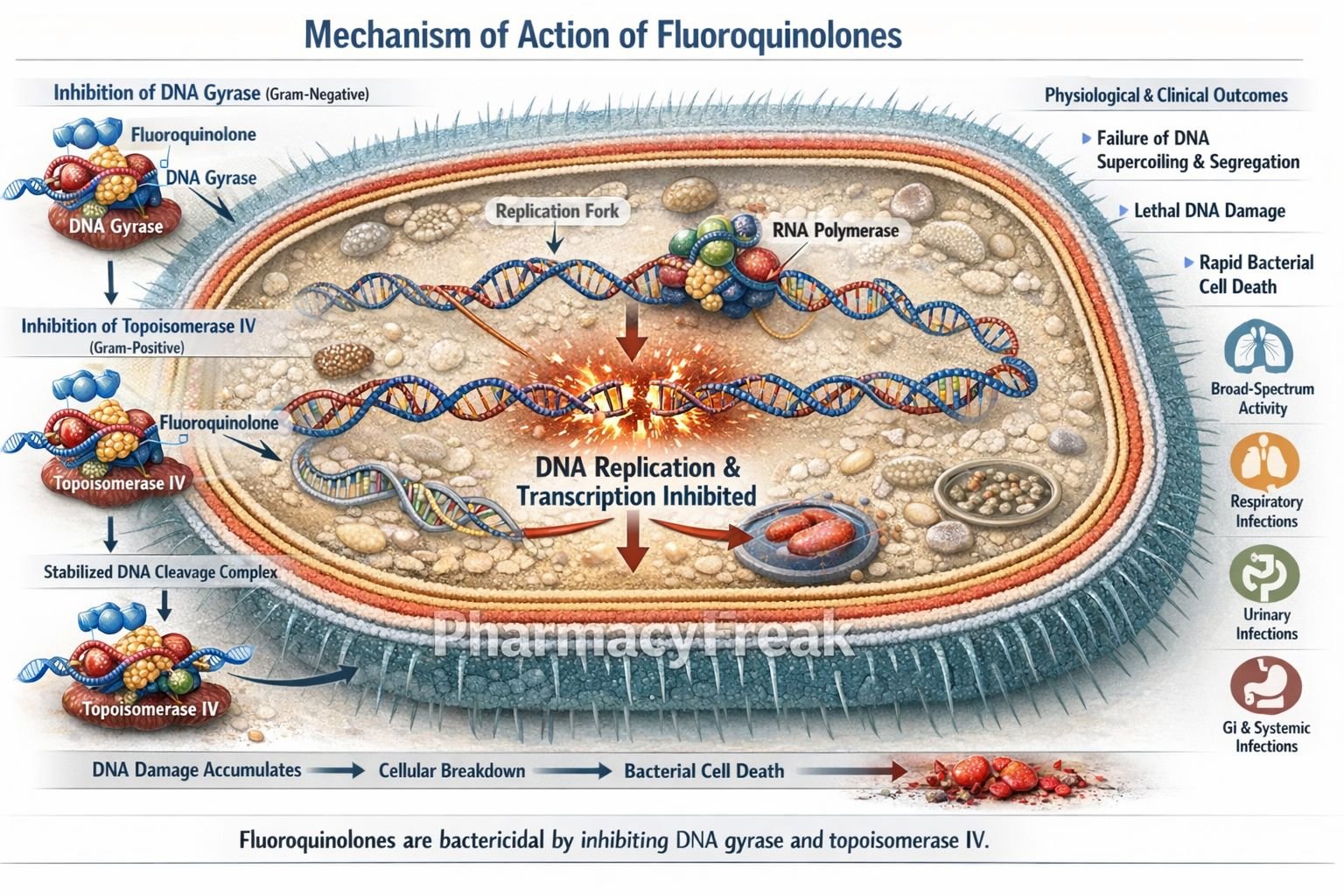
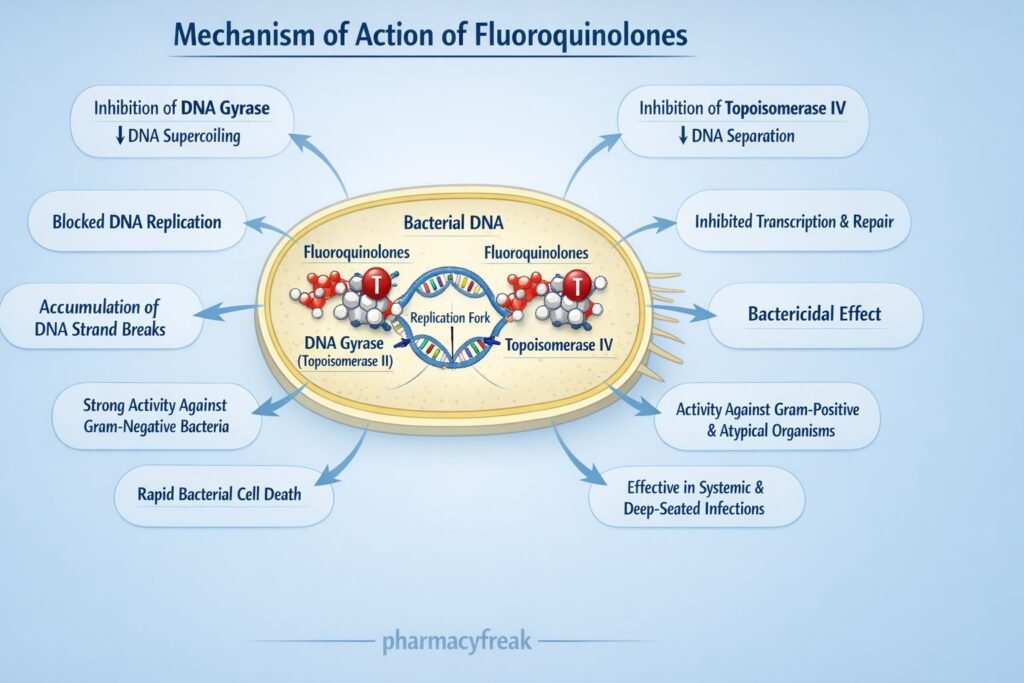
Fluoroquinolones exert bactericidal activity by inhibiting bacterial DNA replication and transcription.
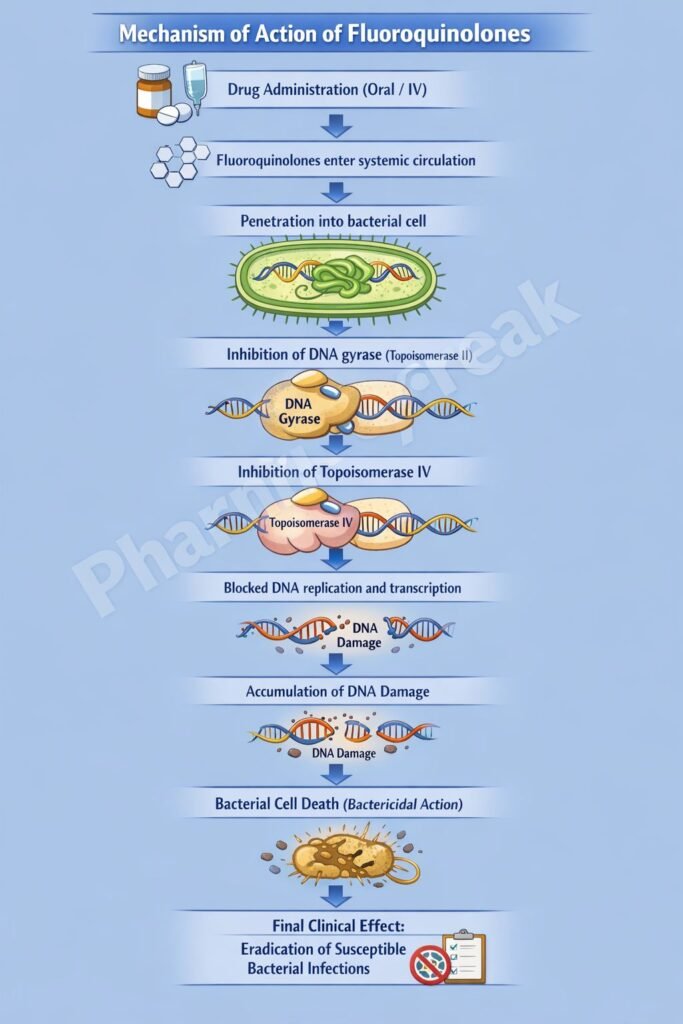
Step 1: Entry into bacterial cell
Fluoroquinolones penetrate bacterial cells through porin channels in gram-negative bacteria and by diffusion in gram-positive bacteria.
Step 2: Inhibition of DNA gyrase (Topoisomerase II)
In gram-negative bacteria, fluoroquinolones primarily inhibit DNA gyrase (topoisomerase II), an enzyme responsible for introducing negative supercoils into DNA.
Step 3: Inhibition of Topoisomerase IV
In gram-positive bacteria, the main target is topoisomerase IV, which is essential for separation of replicated daughter DNA strands.
Step 4: Stabilization of DNA–enzyme complex
Fluoroquinolones stabilize the DNA–topoisomerase complex after DNA cleavage, preventing re-ligation of DNA strands.
Step 5: Accumulation of DNA breaks
Persistent double-strand DNA breaks inhibit DNA replication and transcription.
Step 6: Rapid bacterial cell death
Irreversible DNA damage results in bactericidal, concentration-dependent killing.
Exam pearl:
Fluoroquinolones cause double-strand DNA breaks, similar to topoisomerase II inhibitors in cancer chemotherapy.
Pharmacokinetics
- Route of administration: Oral, IV
- Bioavailability: High (50–100%, drug dependent)
- Distribution: Excellent tissue penetration (lungs, prostate, bone)
- CNS penetration: Moderate
- Protein binding: Variable
- Metabolism: Hepatic (some agents)
- Excretion: Renal (ciprofloxacin, levofloxacin) or hepatic (moxifloxacin)
- Dose adjustment: Required in renal impairment (except moxifloxacin)
Clinical Uses
- Urinary tract infections
- Gastrointestinal infections (e.g., traveler’s diarrhea)
- Respiratory tract infections (CAP, atypical pneumonia)
- Sexually transmitted infections (gonorrhea – resistance dependent)
- Bone and joint infections
- Anthrax prophylaxis and treatment
- Pseudomonas infections (ciprofloxacin)
Adverse Effects
Gastrointestinal:
- Nausea
- Diarrhea
Central nervous system:
- Headache
- Dizziness
- Seizures (rare)
Musculoskeletal (hallmark):
- Tendinitis
- Tendon rupture (Achilles tendon)
- Arthropathy (contraindicated in children)
Cardiac:
- QT interval prolongation (especially moxifloxacin)
Metabolic:
- Dysglycemia (hypo- or hyperglycemia)
Exam warning:
Avoid fluoroquinolones in pregnancy and pediatric patients unless absolutely necessary.
Comparative Analysis
Fluoroquinolones vs β-Lactams vs Macrolides
| Feature | Fluoroquinolones | β-Lactams | Macrolides |
|---|---|---|---|
| Primary target | DNA gyrase / Topo IV | Cell wall synthesis | Protein synthesis (50S) |
| Bactericidal | Yes | Yes | Mostly static |
| Intracellular activity | Good | Poor | Good |
| Post-antibiotic effect | Present | Minimal | Minimal |
| Tendon toxicity | Yes | No | No |
| QT prolongation | Yes | Rare | Yes |
Explanation:
Fluoroquinolones directly target bacterial DNA replication, making them rapidly bactericidal with broad tissue penetration. However, safety concerns limit their routine use compared with β-lactams.
MCQs
- Fluoroquinolones inhibit which enzyme in gram-negative bacteria?
a) Topoisomerase I
b) DNA polymerase
c) DNA gyrase
d) RNA polymerase
Answer: c) DNA gyrase
- Primary target of fluoroquinolones in gram-positive bacteria is:
a) DNA gyrase
b) Topoisomerase IV
c) RNA polymerase
d) Peptidoglycan synthase
Answer: b) Topoisomerase IV
- Nature of antibacterial action of fluoroquinolones is:
a) Bacteriostatic
b) Fungicidal
c) Bactericidal
d) Virucidal
Answer: c) Bactericidal
- Fluoroquinolones cause bacterial death by inducing:
a) Cell wall lysis
b) Single-strand DNA breaks
c) Double-strand DNA breaks
d) Protein misfolding
Answer: c) Double-strand DNA breaks
- Which fluoroquinolone is most active against Pseudomonas?
a) Levofloxacin
b) Moxifloxacin
c) Ciprofloxacin
d) Norfloxacin
Answer: c) Ciprofloxacin
- Tendon rupture with fluoroquinolones most commonly affects the:
a) Patellar tendon
b) Achilles tendon
c) Rotator cuff
d) Biceps tendon
Answer: b) Achilles tendon
- Fluoroquinolones are contraindicated in children due to:
a) Hepatotoxicity
b) Bone marrow suppression
c) Cartilage toxicity
d) Nephrotoxicity
Answer: c) Cartilage toxicity
- QT prolongation is most associated with:
a) Ciprofloxacin
b) Norfloxacin
c) Moxifloxacin
d) Ofloxacin
Answer: c) Moxifloxacin
- Fluoroquinolones show which killing pattern?
a) Time-dependent
b) Concentration-dependent
c) Static effect
d) Immune-mediated
Answer: b) Concentration-dependent
- Resistance to fluoroquinolones commonly occurs due to:
a) β-lactamase production
b) Altered ribosomal binding
c) Mutation in DNA gyrase
d) Reduced peptidoglycan synthesis
Answer: c) Mutation in DNA gyrase
FAQs
1. Why are fluoroquinolones bactericidal?
They cause irreversible DNA damage.
2. Why are they avoided in children?
Due to cartilage and tendon toxicity.
3. Do fluoroquinolones work against atypical organisms?
Yes, they have good intracellular penetration.
4. Which fluoroquinolone has best respiratory coverage?
Levofloxacin and moxifloxacin.
5. Why should antacids be avoided with fluoroquinolones?
They reduce absorption by chelation.
References
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics
https://accesspharmacy.mhmedical.com - Katzung BG. Basic and Clinical Pharmacology
https://accessmedicine.mhmedical.com - Tripathi KD. Essentials of Medical Pharmacology
- Harrison’s Principles of Internal Medicine
https://accessmedicine.mhmedical.com

