Table of Contents
Introduction
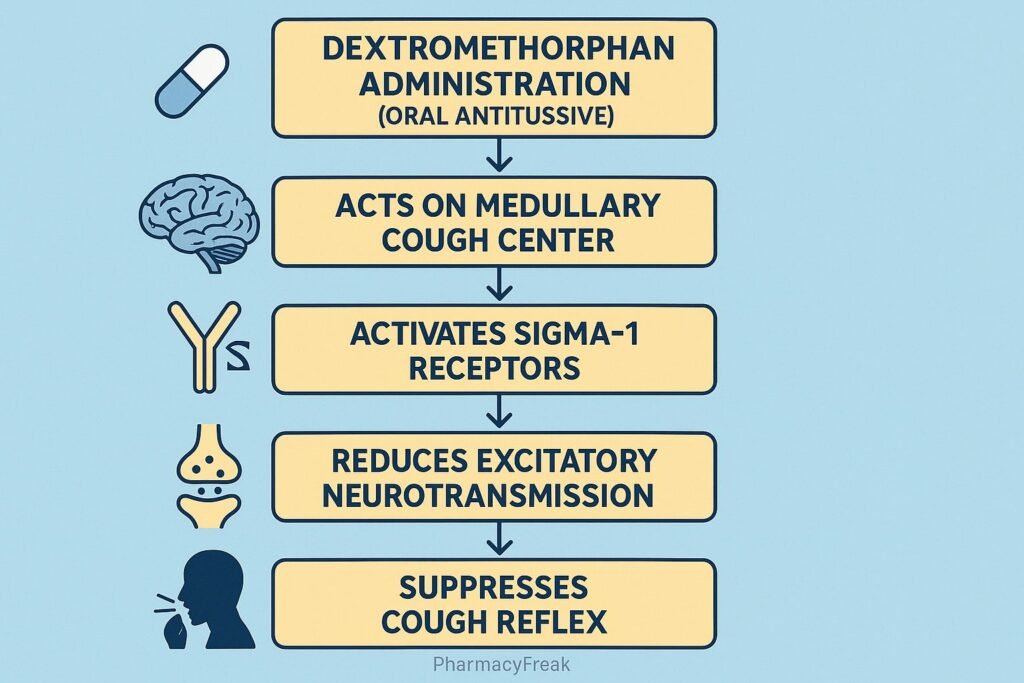
Dextromethorphan is a widely used antitussive (cough suppressant) agent found in over-the-counter cold and cough formulations. Mechanism of Action of Dextromethorphan involves modulation of the central nervous system by acting on multiple receptors, including NMDA, sigma-1, and serotonin transporters. Beyond cough suppression, it has emerging roles in neurology and psychiatry, such as treatment of pseudobulbar affect and adjunctive use in major depressive disorder. Understanding its pharmacological mechanism provides insights into its therapeutic applications and potential risks.
Mechanism of Action (Step-wise)
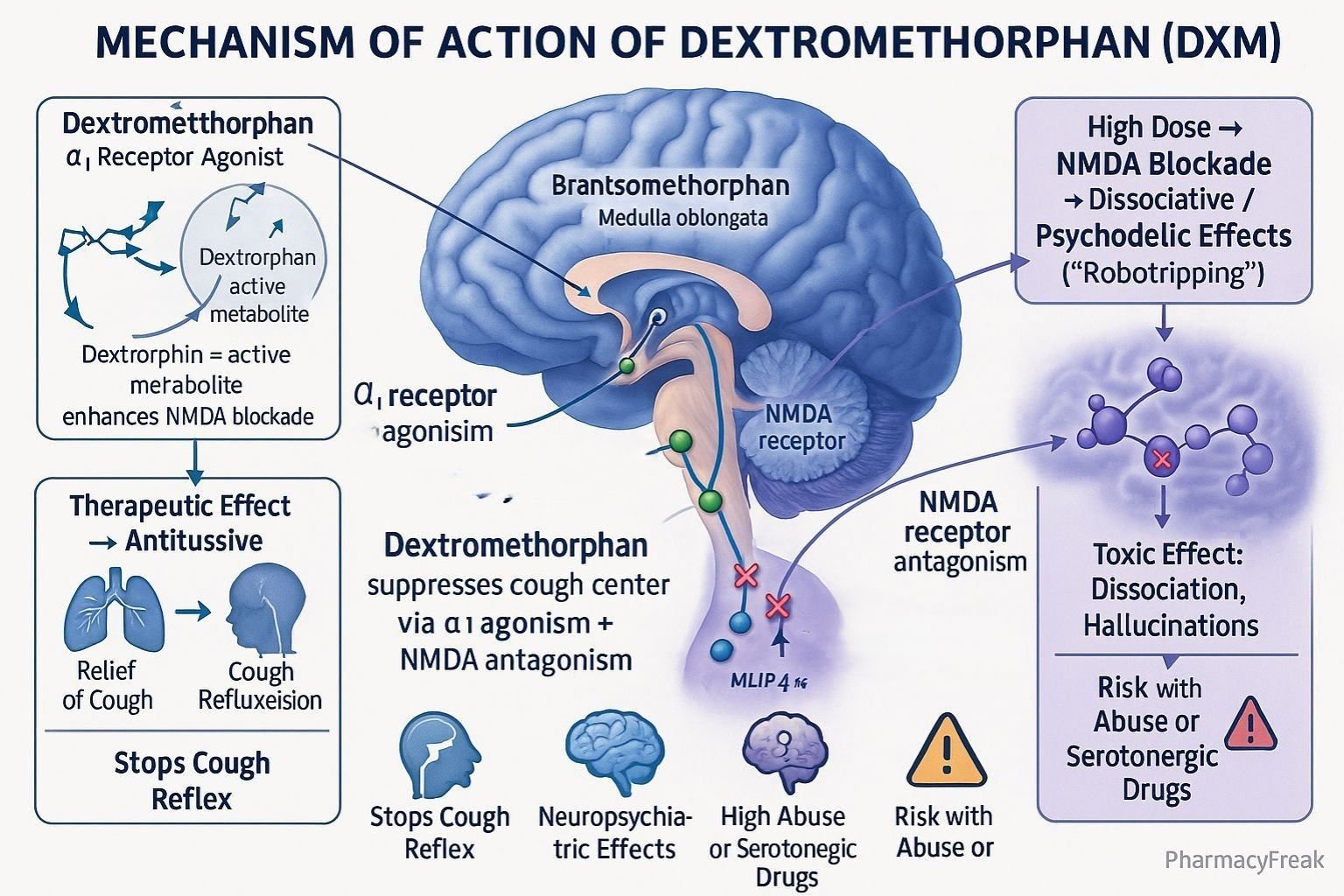
- NMDA Receptor Antagonism
- Dextromethorphan and its active metabolite (dextrorphan) act as non-competitive antagonists of the N-methyl-D-aspartate (NMDA) receptor.
- This reduces excitatory glutamate signaling in the brain.
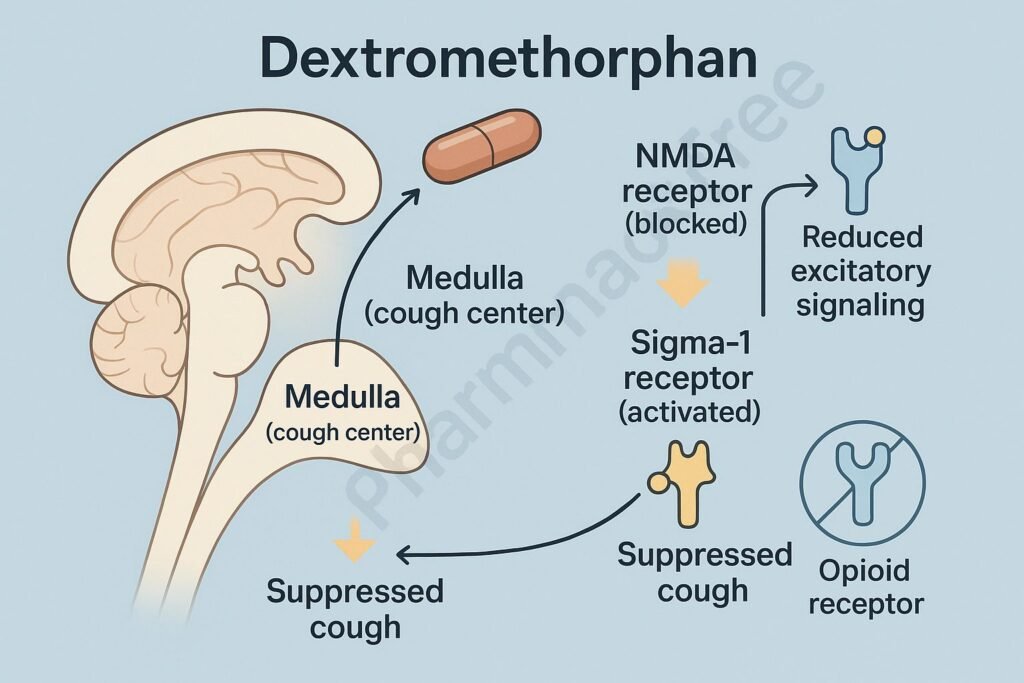
- Sigma-1 Receptor Agonism
- Binds to sigma-1 receptors in the brain.
- Modulates neuronal excitability and contributes to its antitussive and neuroprotective properties.
- Serotonin and Norepinephrine Reuptake Inhibition
- Weakly inhibits reuptake of serotonin and norepinephrine.
- Enhances mood and contributes to central effects.
- Cough Suppression
- Acts on the medullary cough center, raising the threshold for cough reflex.
- Overall Effect
- Suppresses cough reflex.
- Modulates CNS pathways, producing therapeutic and sometimes dissociative effects at higher doses.
Pharmacokinetics
- Absorption: Rapid oral absorption.
- Distribution: Wide distribution; crosses blood–brain barrier.
- Metabolism: Extensively metabolized in the liver via CYP2D6 into dextrorphan (active metabolite).
- Excretion: Primarily renal excretion.
- Half-life: 3–6 hours (variable depending on metabolism).
Clinical Uses
- Suppression of non-productive cough.
- Pseudobulbar affect (in combination with quinidine).
- Investigated in treatment-resistant depression (as part of dextromethorphan–bupropion combination).
- Off-label uses: certain neuropathic pain conditions.
Adverse Effects
- Common: Drowsiness, dizziness, nausea, gastrointestinal upset.
- Less common: Confusion, blurred vision, dry mouth.
- Serious (high doses): Dissociation, hallucinations, serotonin syndrome (with serotonergic drugs), respiratory depression.
- Abuse potential: At supratherapeutic doses, produces dissociative and hallucinogenic effects similar to phencyclidine (PCP) and ketamine.
Comparative Analysis
| Feature | Dextromethorphan | Codeine | Benzonatate |
|---|---|---|---|
| Mechanism | NMDA antagonist, sigma-1 agonist, antitussive | μ-opioid agonist, antitussive | Anesthetizes stretch receptors |
| Abuse potential | Moderate (at high doses) | High | Low |
| Respiratory depression | Low at therapeutic doses | Significant risk | Minimal |
| Clinical uses | Cough, pseudobulbar affect, depression (adjunct) | Cough, pain relief | Cough only |
| OTC availability | Yes | No (controlled) | Prescription only |
MCQs
1. Dextromethorphan is primarily used as a:
a) Analgesic
b) Antitussive
c) Anxiolytic
d) Antidepressant
Answer: b) Antitussive
2. Which receptor is antagonized by dextromethorphan?
a) GABA-A receptor
b) NMDA receptor
c) Dopamine D2 receptor
d) AMPA receptor
Answer: b) NMDA receptor
3. Dextromethorphan is metabolized by which enzyme?
a) CYP3A4
b) CYP2C19
c) CYP2D6
d) CYP1A2
Answer: c) CYP2D6
4. High doses of dextromethorphan may cause:
a) Sedation only
b) Dissociation and hallucinations
c) Severe hypertension
d) Bradycardia
Answer: b) Dissociation and hallucinations
5. Dextromethorphan is contraindicated with which class of drugs?
a) NSAIDs
b) MAO inhibitors
c) Beta-blockers
d) Calcium channel blockers
Answer: b) MAO inhibitors
6. Which receptor is involved in dextromethorphan’s neuroprotective effects?
a) Sigma-1 receptor
b) Dopamine D1 receptor
c) H1 receptor
d) Muscarinic receptor
Answer: a) Sigma-1 receptor
7. The active metabolite of dextromethorphan is:
a) Morphine
b) Norcodeine
c) Dextrorphan
d) Hydroxymorphone
Answer: c) Dextrorphan
8. Which adverse effect is associated with dextromethorphan abuse?
a) Arrhythmia
b) Hallucinations
c) Agranulocytosis
d) Nephrotoxicity
Answer: b) Hallucinations
9. In pseudobulbar affect, dextromethorphan is combined with:
a) Fluoxetine
b) Quinidine
c) Bupropion
d) Clonazepam
Answer: b) Quinidine
10. The half-life of dextromethorphan is approximately:
a) 1 hour
b) 3–6 hours
c) 12–18 hours
d) 24 hours
Answer: b) 3–6 hours
FAQs
Q1. Is dextromethorphan addictive?
At normal doses, no. At high doses, it can be abused for dissociative effects.
Q2. Can dextromethorphan be used with MAO inhibitors?
No, this combination can lead to serotonin syndrome.
Q3. What is the active metabolite of dextromethorphan?
Dextrorphan, which contributes to NMDA receptor antagonism.
Q4. Is dextromethorphan safe for children?
It is generally not recommended in children under 6 years due to risk of side effects.
Q5. Can dextromethorphan be used in depression?
Yes, in combination formulations (e.g., with bupropion) it has shown antidepressant effects.
Q6. What happens in dextromethorphan overdose?
Confusion, hallucinations, dissociation, ataxia, and rarely respiratory depression.
References
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics
- Katzung Basic and Clinical Pharmacology
- FDA Prescribing Information on Dextromethorphan
- Stahl’s Essential Psychopharmacology

