Table of Contents
Introduction
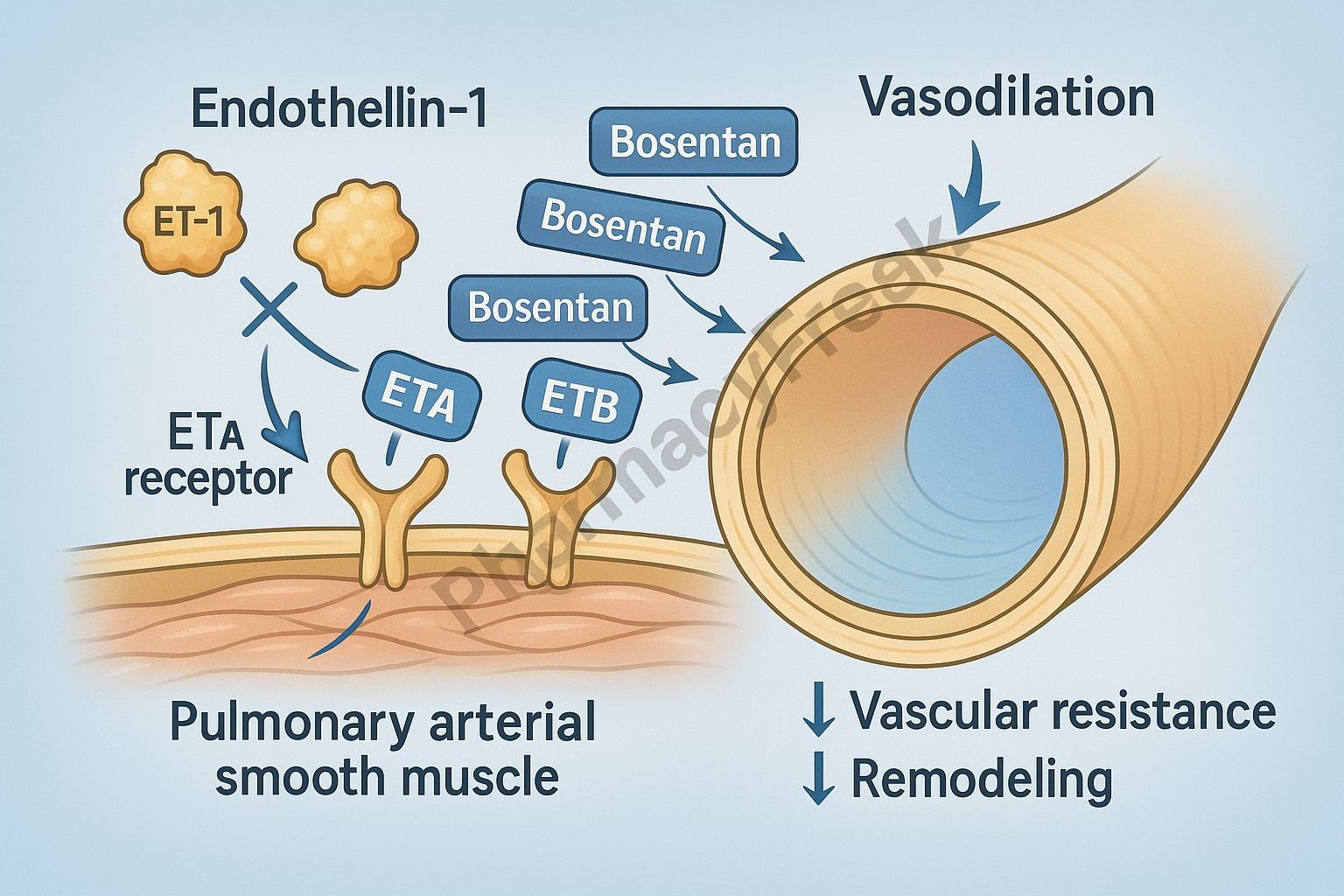
Bosentan is an oral endothelin receptor antagonist (ERA) used primarily for the treatment of pulmonary arterial hypertension (PAH). Endothelin-1 (ET-1) is one of the most potent vasoconstrictors in the human body, and its overactivity plays a central role in the pathophysiology of PAH by causing vasoconstriction, vascular hypertrophy, smooth muscle proliferation, and fibrosis.
Bosentan works by blocking both ETA and ETB receptors, reducing pulmonary vascular resistance and improving exercise capacity, functional class, and long-term outcomes in PAH patients.


Mechanism of Action (Step-wise)
1. Dual Endothelin Receptor Blockade (ETA and ETB) – Primary Mechanism
Bosentan is a competitive antagonist of:
- ETA receptors (primary mediators of vasoconstriction)
- ETB receptors (involved in clearance of ET-1 and vasodilation)
Blocking these receptors prevents endothelin-1 from binding.
2. Inhibition of ETA Receptors → Reduced Vasoconstriction
ETA receptors are located on vascular smooth muscle cells.
Endothelin binding normally causes:
- Vasoconstriction
- Proliferation of smooth muscle
- Fibrosis
- Hypertrophy
Bosentan blocks this action →
- ↓ Vasoconstriction
- ↓ Vascular remodeling
- ↓ Pulmonary arterial pressure
3. Blockade of ETB Receptors → Reduced ET-1 Levels
ETB receptors are responsible for:
- ET-1 clearance
- Nitric oxide (NO) release
- Prostacyclin release
Bosentan blocks ETB receptors, causing:
- ↓ ET-1 clearance → ↑ plasma ET-1 levels
- But therapeutic effect still dominated by ETA inhibition
- Some reduction in vasodilation due to ETB blockade
However, overall effect remains strongly vasodilatory because ETA blockade is dominant.
4. Reduction in Pulmonary Vascular Resistance
By decreasing both vasoconstrictive and proliferative pathways, bosentan:
- ↓ Pulmonary arterial pressure
- ↓ Right ventricular workload
- ↑ Exercise tolerance
- Improves WHO functional class
5. Antiproliferative Effects
Bosentan inhibits endothelin-1 stimulated:
- Smooth muscle cell proliferation
- Fibroblast activation
- Vascular remodeling
This slows disease progression at the structural level.
6. Summary of Mechanism
| Mechanism | Effect |
|---|---|
| ETA receptor blockade | ↓ Vasoconstriction, ↓ proliferation |
| ETB receptor blockade | ↑ ET-1 levels, mild ↓ vasodilation |
| ↓ Smooth muscle growth | ↓ Remodeling |
| ↓ Pulmonary vascular resistance | Improved PAH symptoms |
| ↓ Right heart strain | Better functional capacity |
Pharmacokinetics
- Absorption: Good oral absorption
- Bioavailability: ~50%
- Distribution: Highly protein bound
- Metabolism: Hepatic (CYP2C9, CYP3A4)
- Half-life: 5–6 hours
- Elimination: Biliary
Clinical Uses
- Primary pulmonary arterial hypertension (PAH)
- PAH associated with connective tissue disease
- Eisenmenger syndrome (select cases)
- Off-label: digital ulcers in scleroderma
Adverse Effects
- Elevated liver enzymes (major toxicity)
- Peripheral edema
- Anemia
- Hypotension
- Headache
- Flushing
- Nasal congestion
- Teratogenicity (contraindicated in pregnancy)
Contraindications
- Pregnancy (Category X)
- Moderate to severe hepatic impairment
- Use with cyclosporine or glyburide
- Severe anemia
Comparative Analysis
| Feature | Bosentan | Ambrisentan | Macitentan |
|---|---|---|---|
| Receptor selectivity | ETA + ETB (dual) | ETA selective | Dual, more potent |
| Liver toxicity | High | Lower | Lower |
| Dosing | Twice daily | Once daily | Once daily |
| Drug interactions | More frequent | Fewer | Moderate |
MCQs
1. Bosentan works primarily by blocking:
a) Calcium channels
b) Beta-2 receptors
c) Endothelin receptors
d) Alpha-1 receptors
Answer: c) Endothelin receptors
2. ETA receptor blockade results in:
a) Increased vasoconstriction
b) Decreased smooth muscle proliferation
c) Increased fibrosis
d) Reduced NO production
Answer: b) Decreased smooth muscle proliferation
3. The major toxicity of bosentan is:
a) Nephrotoxicity
b) Hepatotoxicity
c) Cardiotoxicity
d) Pulmonary fibrosis
Answer: b) Hepatotoxicity
4. Bosentan increases plasma endothelin levels by blocking:
a) ETA receptors
b) ETB receptors
c) Beta-1 receptors
d) P-glycoprotein
Answer: b) ETB receptors
5. Bosentan is primarily used in:
a) Asthma
b) Pulmonary arterial hypertension
c) Hypertension crisis
d) COPD
Answer: b) Pulmonary arterial hypertension
FAQs
Q1. Why does bosentan require monthly liver monitoring?
Because it commonly causes dose-dependent hepatotoxicity.
Q2. Does bosentan improve survival in PAH?
Yes—by reducing pulmonary pressures and preventing right heart failure.
Q3. Can bosentan be used in pregnancy?
No—it is highly teratogenic.
Q4. What class of drug is bosentan?
A dual endothelin receptor antagonist.
Q5. How long does bosentan take to work?
Improvements are typically seen within 4–8 weeks.
References
Goodman & Gilman’s Pharmacological Basis of Therapeutics
https://accesspharmacy.mhmedical.com/book.aspx?bookid=2189
Katzung: Basic & Clinical Pharmacology
https://accessmedicine.mhmedical.com/book.aspx?bookid=2464
Tripathi: Essentials of Medical Pharmacology
https://jaypeebrothers.com/
Harrison’s Principles of Internal Medicine
https://accessmedicine.mhmedical.com/book.aspx?bookid=2129
