Table of Contents
Introduction
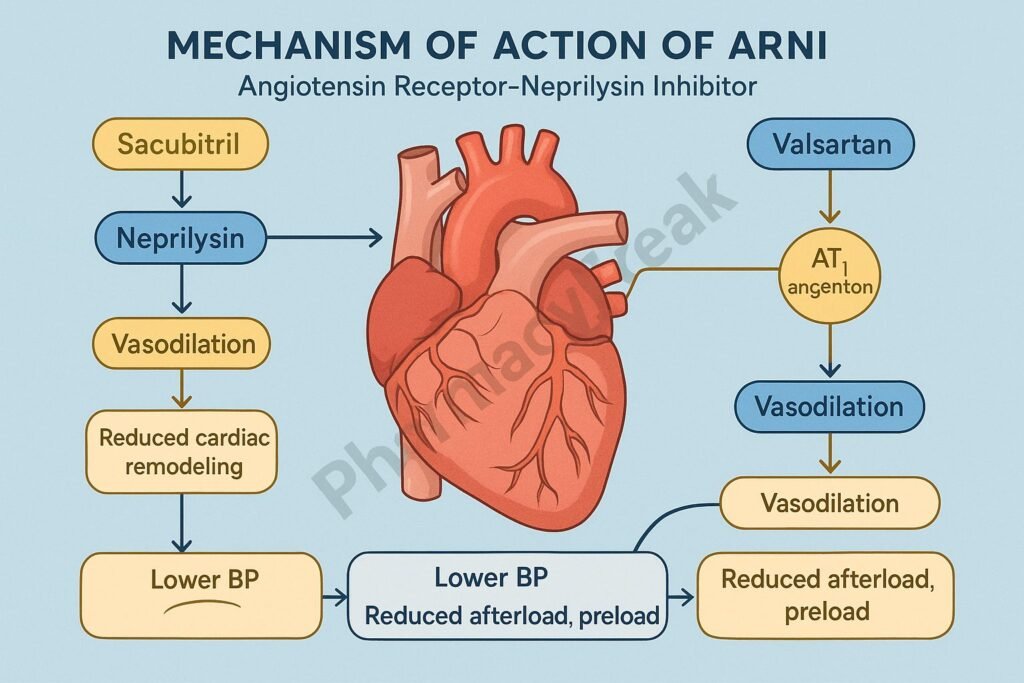
ARNI (Angiotensin Receptor–Neprilysin Inhibitor) represents a major advancement in the treatment of heart failure with reduced ejection fraction (HFrEF). The most widely used ARNI is the fixed-dose combination Sacubitril/Valsartan, marketed as Entresto.
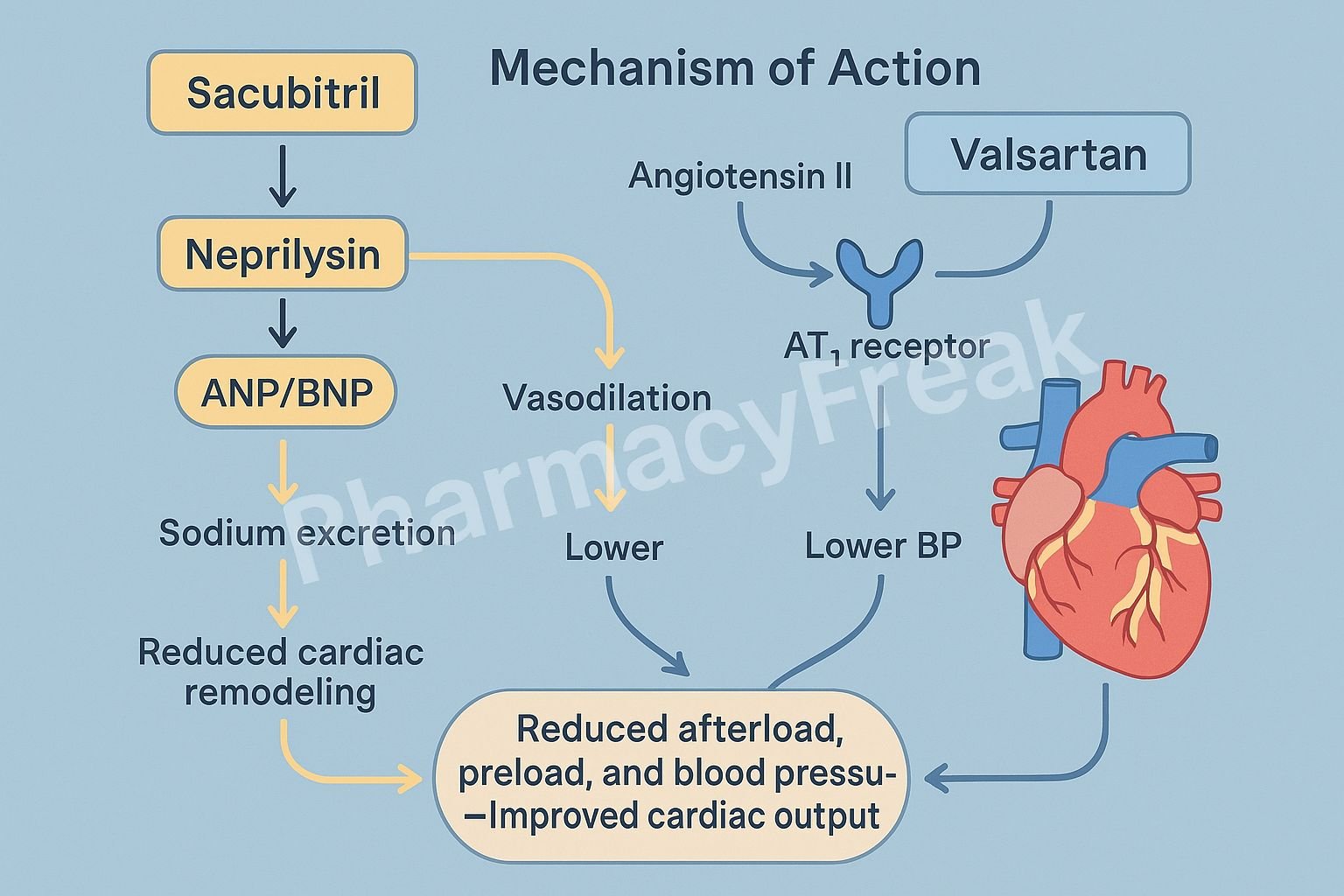
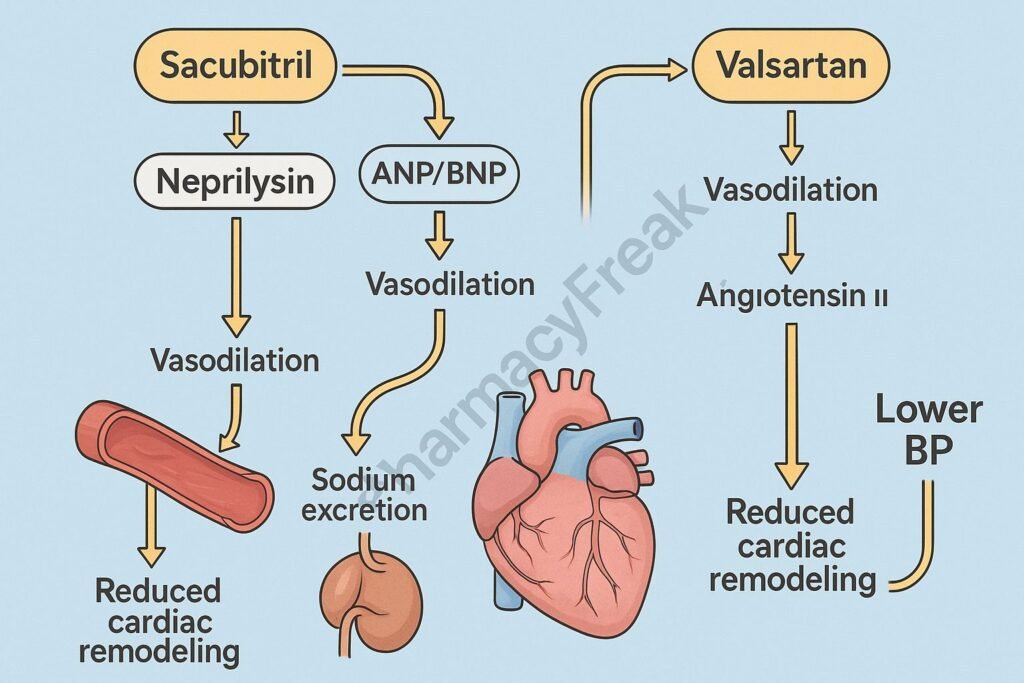
Mechanism of Action of ARNI involves dual inhibition of the renin–angiotensin–aldosterone system (RAAS) and the neprilysin (neutral endopeptidase) pathway. This unique mechanism enhances natriuretic peptide activity while simultaneously blocking the harmful effects of angiotensin II, resulting in vasodilation, natriuresis, and improved cardiac remodeling.
Mechanism of Action (Step-wise)
1. Inhibition of Neprilysin (Sacubitril Component)
- Mechanism:
- Sacubitril is a prodrug converted to sacubitrilat, which inhibits neprilysin, the enzyme responsible for degrading several vasoactive peptides.
- These peptides include natriuretic peptides (ANP, BNP), bradykinin, and adrenomedullin.
- Inhibiting neprilysin increases levels of these beneficial substances, leading to vasodilation and natriuresis.
- Effects:
- ↑ Vasodilation → ↓ Systemic vascular resistance
- ↑ Natriuresis and diuresis → ↓ Preload and afterload
- ↓ Cardiac fibrosis and hypertrophy
- ↑ Glomerular filtration and renal perfusion
2. Blockade of Angiotensin II Type 1 (AT₁) Receptors (Valsartan Component)
- Mechanism:
- Valsartan, an angiotensin II receptor blocker (ARB), selectively blocks AT₁ receptors, thereby inhibiting the harmful effects of angiotensin II.
- This prevents vasoconstriction, aldosterone release, and sodium retention.
- It also inhibits cardiac remodeling and hypertrophy associated with chronic heart failure.
- Effects:
- ↓ Vasoconstriction → ↓ Afterload
- ↓ Aldosterone → ↓ Sodium and water retention → ↓ Preload
- ↓ Myocardial fibrosis → Improved cardiac function
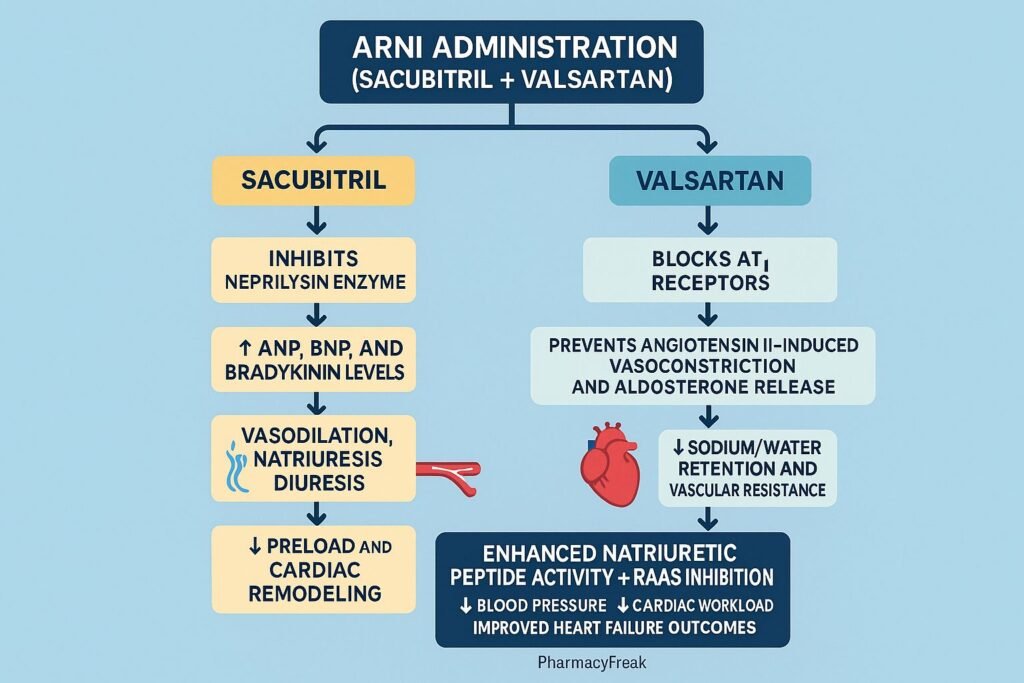
3. Combined (Synergistic) Mechanism of ARNI
The combination of neprilysin inhibition (Sacubitril) and AT₁ receptor blockade (Valsartan) produces a balanced neurohormonal modulation, enhancing beneficial effects while suppressing maladaptive responses in heart failure.
| Pathway | Effect of ARNI |
|---|---|
| Natriuretic Peptides | ↑ Natriuresis, diuresis, vasodilation |
| RAAS Inhibition | ↓ Vasoconstriction, ↓ aldosterone |
| Bradykinin | ↑ Vasodilatory and cardioprotective effects |
| Cardiac Remodeling | ↓ Fibrosis, ↓ hypertrophy |
| Blood Pressure | ↓ Systemic vascular resistance, ↓ preload/afterload |
4. Summary of Molecular Actions
- Sacubitril (Neprilysin inhibitor): Increases endogenous vasodilators (ANP, BNP, bradykinin).
- Valsartan (AT₁ blocker): Reduces vasoconstrictor and aldosterone-mediated effects.
- Overall Outcome:
- ↓ Blood pressure
- ↓ Cardiac wall stress
- ↓ Sympathetic activation
- ↑ Cardiac output
- Improved survival in heart failure patients
Clinical Uses
- Primary Use: Heart failure with reduced ejection fraction (HFrEF).
- Secondary Use (Under investigation): Heart failure with preserved ejection fraction (HFpEF) and hypertension.
Guideline Recommendation:
- According to ACC/AHA/HFSA Heart Failure Guidelines, ARNI is first-line therapy in symptomatic HFrEF, replacing ACE inhibitors or ARBs, unless contraindicated.
Pharmacokinetics
- Sacubitril: Oral prodrug → converted to sacubitrilat (active metabolite).
- Valsartan: Directly active; oral bioavailability ~25%.
- Onset: 1–2 hours.
- Half-life: Sacubitrilat ~12 hours; Valsartan ~9 hours.
- Excretion: Renal (52%) and fecal (48%).
Adverse Effects
- Common: Hypotension, dizziness, hyperkalemia, renal impairment.
- Serious: Angioedema (increased bradykinin).
- Contraindications:
- Concomitant use with ACE inhibitors (must allow ≥36-hour washout period).
- Pregnancy, bilateral renal artery stenosis, history of angioedema.
Comparative Table
| Feature | ACE Inhibitors | ARBs | ARNI (Sacubitril/Valsartan) |
|---|---|---|---|
| Mechanism | ↓ Ang II formation | Block AT₁ receptor | Block AT₁ + Inhibit Neprilysin |
| Bradykinin Effect | ↑ | ↔ | ↑↑ |
| Vasodilation | Moderate | Moderate | Marked |
| Natriuresis | Minimal | Minimal | Significant |
| Cardiac Remodeling | ↓ | ↓ | Strong ↓↓ |
| Adverse Effects | Cough, hyperkalemia | Hyperkalemia | Hypotension, angioedema |
| Heart Failure Benefit | Proven | Proven | Superior to ACEI (PARADIGM-HF Trial) |
MCQs
1. ARNI stands for:
a) Angiotensin Receptor–Nitric Inhibitor
b) Angiotensin Receptor–Neprilysin Inhibitor
c) Angiotensin–Renin Nephron Inhibitor
d) Aldosterone Receptor–Nephron Inhibitor
Answer: b) Angiotensin Receptor–Neprilysin Inhibitor
2. Sacubitril inhibits which enzyme?
a) ACE
b) Neprilysin
c) Aldosterone synthase
d) Renin
Answer: b) Neprilysin
3. The main pharmacological effect of neprilysin inhibition is:
a) Decreased natriuretic peptides
b) Increased vasoconstriction
c) Increased vasodilator peptides (ANP, BNP)
d) Increased angiotensin II
Answer: c) Increased vasodilator peptides (ANP, BNP)
4. Valsartan acts by blocking:
a) AT₂ receptors
b) AT₁ receptors
c) β₁ receptors
d) M₂ receptors
Answer: b) AT₁ receptors
5. Major adverse effect of ARNI therapy is:
a) Cough
b) Hypotension and angioedema
c) Bradycardia
d) Hypokalemia
Answer: b) Hypotension and angioedema
6. Sacubitril/Valsartan should not be used with:
a) Calcium channel blockers
b) ACE inhibitors
c) Diuretics
d) Nitrates
Answer: b) ACE inhibitors
7. Neprilysin inhibition increases levels of:
a) Angiotensin II
b) Natriuretic peptides and bradykinin
c) Vasopressin
d) Endothelin
Answer: b) Natriuretic peptides and bradykinin
8. Clinical indication for ARNI is:
a) Acute coronary syndrome
b) Heart failure with reduced ejection fraction
c) Hypertension only
d) Stable angina
Answer: b) Heart failure with reduced ejection fraction
9. Sacubitril is converted to:
a) Sacubitrilat
b) Sacubrin
c) Valsartate
d) Neprilate
Answer: a) Sacubitrilat
10. The combination of ARNI provides:
a) Only vasodilation
b) Vasodilation + natriuresis + neurohormonal balance
c) Only diuresis
d) Aldosterone stimulation
Answer: b) Vasodilation + natriuresis + neurohormonal balance
FAQs
Q1. What is the main advantage of ARNI over ACE inhibitors?
ARNI provides dual neurohormonal modulation, improving survival and reducing hospitalization more effectively than ACE inhibitors.
Q2. Why must ACE inhibitors be discontinued before starting ARNI?
Because both increase bradykinin levels, concurrent use raises the risk of angioedema.
Q3. How does ARNI affect cardiac remodeling?
It reduces fibrosis and hypertrophy, promoting reverse remodeling and improved ventricular function.
Q4. What is the recommended washout period between ACE inhibitor and ARNI?
At least 36 hours to prevent angioedema.
Q5. What trial established ARNI’s clinical superiority?
The PARADIGM-HF Trial, which showed significant mortality reduction compared to enalapril.
References
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics
- Katzung BG. Basic and Clinical Pharmacology
- Tripathi KD. Essentials of Medical Pharmacology
- Harrison’s Principles of Internal Medicine
- McMurray JJ et al., NEJM 2014;371:993–1004 (PARADIGM-HF Trial)


