
Table of Contents
Introduction
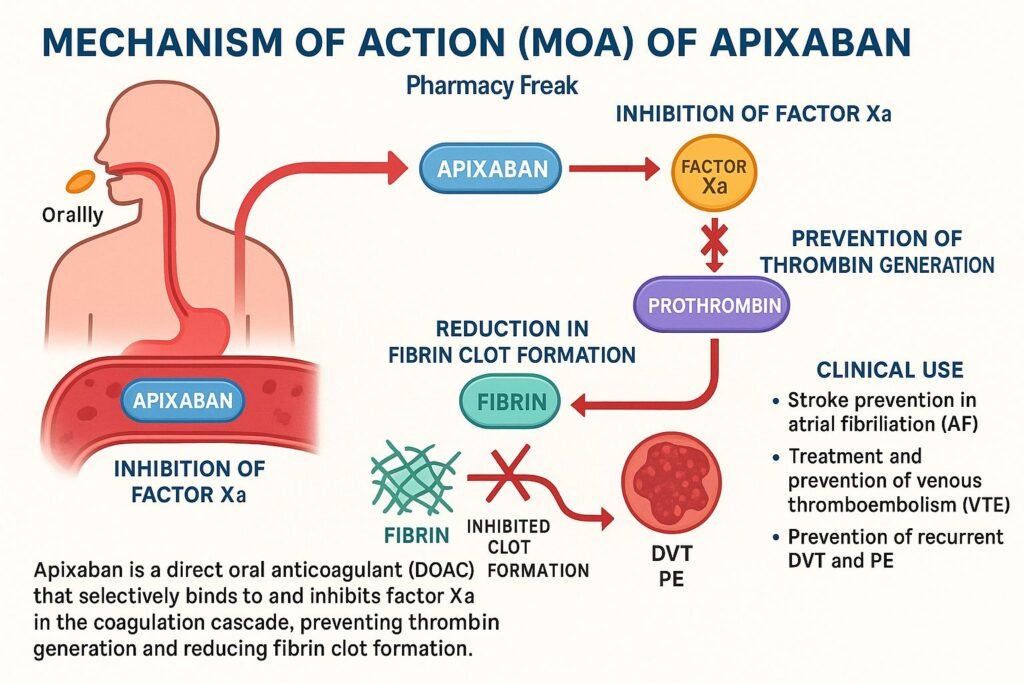
Apixaban is a direct oral anticoagulant (DOAC) used to prevent and treat thrombosis. It is specifically indicated for stroke prevention in non-valvular atrial fibrillation, treatment and prevention of venous thromboembolism (VTE), and management of deep vein thrombosis (DVT) and pulmonary embolism (PE). Its predictable pharmacokinetics and oral administration make it a widely used alternative to warfarin.
Step-by-Step Mechanism of Action
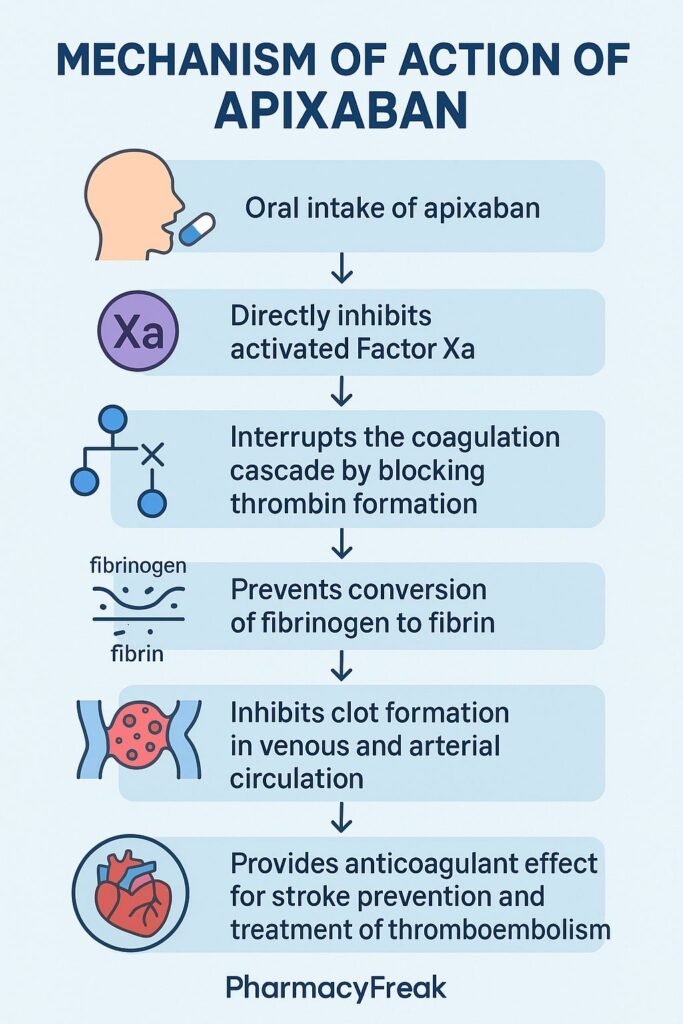
- Selective Factor Xa Inhibition
Apixaban directly and reversibly inhibits both free and clot-bound factor Xa, without requiring antithrombin III. - Prevention of Prothrombinase Activity
By blocking factor Xa, apixaban disrupts the prothrombinase complex, which converts prothrombin to thrombin. - Reduced Thrombin Generation
With less thrombin produced, the conversion of fibrinogen to fibrin is inhibited, limiting clot formation and growth. - Antithrombotic Effect
Blocking the central step in coagulation cascade prevents both arterial and venous thrombus development. - No Direct Platelet Effect
Apixaban does not directly affect platelets, but reduces thrombin-mediated platelet activation indirectly.
Pharmacokinetic Parameters
| Parameter | Value |
|---|---|
| Route | Oral, twice daily |
| Bioavailability | ~50% |
| Time to Peak (Tmax) | ~3–4 hours |
| Protein Binding | ~87% |
| Metabolism | Hepatic via CYP3A4 and CYP1A2 |
| Half-life | ~12 hours |
| Excretion | ~27% renal, remainder via fecal/biliary |
Clinical Uses
- Stroke prevention in non-valvular atrial fibrillation
- Treatment and secondary prevention of DVT/PE
- VTE prophylaxis post-hip or knee replacement surgery
Adverse Effects
- Increased risk of bleeding (most common)
- Minor: Bruising, epistaxis
- Major: Gastrointestinal bleeding, intracranial hemorrhage (less common than warfarin)
- Rare: Hypersensitivity, elevated liver enzymes
Comparative Analysis
| Agent | Factor Xa Inhibition | Monitoring | Reversal Agent |
|---|---|---|---|
| Apixaban | Direct, reversible | No | Andexanet alfa |
| Rivaroxaban | Direct, reversible | No | Andexanet alfa |
| Warfarin | Indirect (VKOR) | Yes (INR) | Vitamin K, PCCs |
MCQs
- Apixaban acts by inhibiting which factor?
a) Thrombin (IIa)
b) Factor Xa
c) Factor VIIa
d) Factor IXa
Answer: b) Factor Xa - It inhibits factor Xa in:
a) Free form
b) Clot-bound form
c) Both
d) Neither
Answer: c) Both - Apixaban requires which cofactor for activity?
a) Antithrombin III
b) Calcium
c) Vitamin K
d) None
Answer: d) None - Reduction in thrombin leads to:
a) Increased fibrin formation
b) Decreased clot formation
c) Platelet aggregation activation
d) Increased coagulation
Answer: b) Decreased clot formation - Which describes apixaban’s effect on platelets?
a) Direct inhibitor
b) Activator
c) No direct effect
d) Irreversible binding
Answer: c) No direct effect - Apixaban’s half-life is approximately:
a) 4 hours
b) 7 hours
c) 12 hours
d) 24 hours
Answer: c) 12 hours - What percentage is excreted renally?
a) ~10%
b) ~27%
c) ~50%
d) >70%
Answer: b) ~27% - The antidote for apixaban bleeding is:
a) Vitamin K
b) Protamine
c) Andexanet alfa
d) Fresh frozen plasma
Answer: c) Andexanet alfa - Compared to warfarin, apixaban requires:
a) Regular INR monitoring
b) Fixed dosing without monitoring
c) Frequent dose adjustments
d) Dietary restrictions
Answer: b) Fixed dosing without monitoring - The time to peak plasma levels is:
a) 1 hour
b) 3–4 hours
c) 8 hours
d) 24 hours
Answer: b) 3–4 hours
FAQs
1. Is routine monitoring needed with apixaban?
No—fixed dosing eliminates the need for INR testing.
2. Can apixaban be used in renal impairment?
Yes—but dose adjustments are required when eGFR <30 mL/min.
3. How long before surgery should apixaban be stopped?
Typically, 24–48 hours before, depending on bleeding risk and renal function.
4. Does apixaban interact with other medications?
Yes—CYP3A4 and P-gp inhibitors or inducers may require dose adjustment.
5. Is the bleeding risk lower than warfarin?
Apixaban has been shown to reduce major and intracranial bleeding compared to warfarin.

