Table of Contents
Introduction
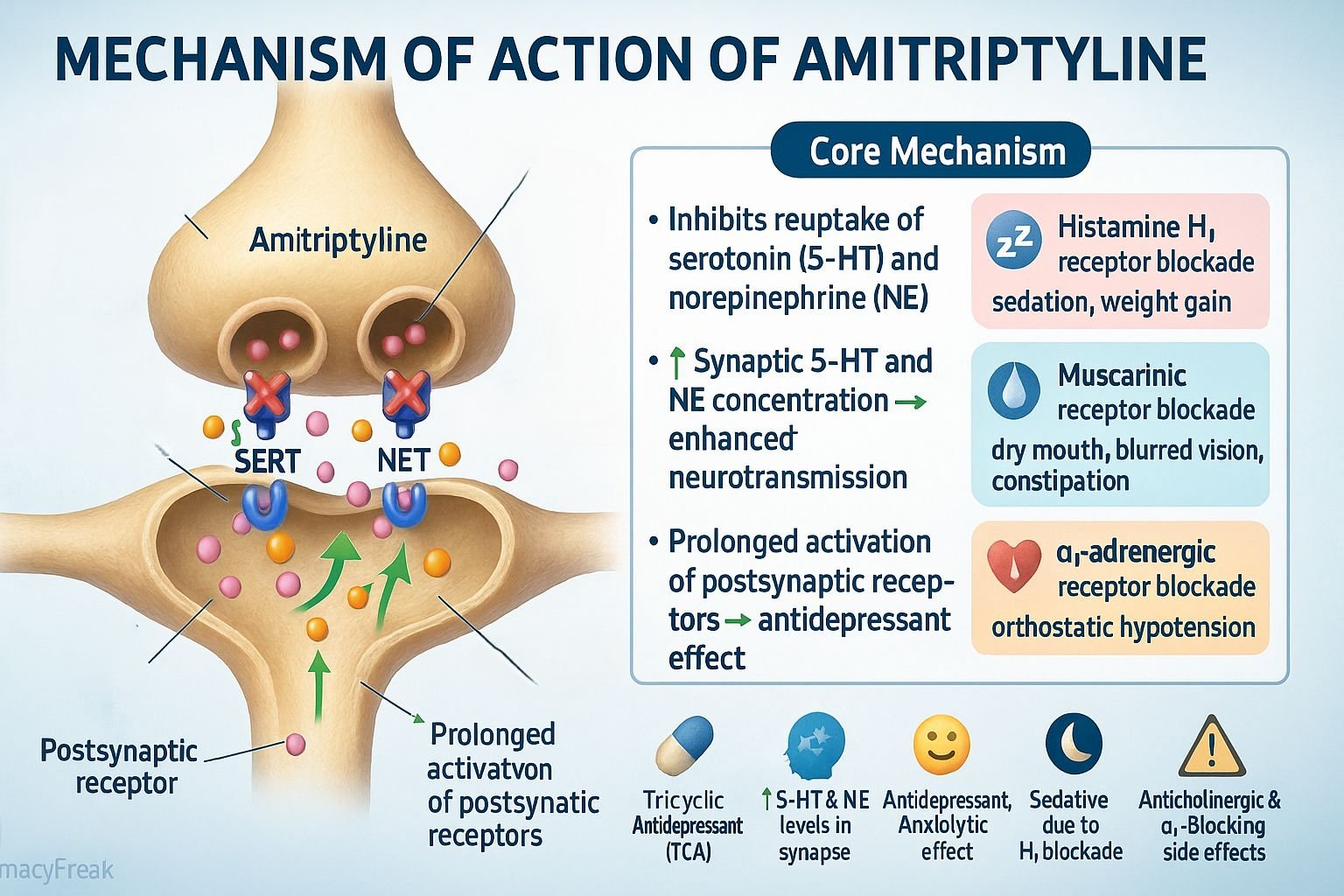
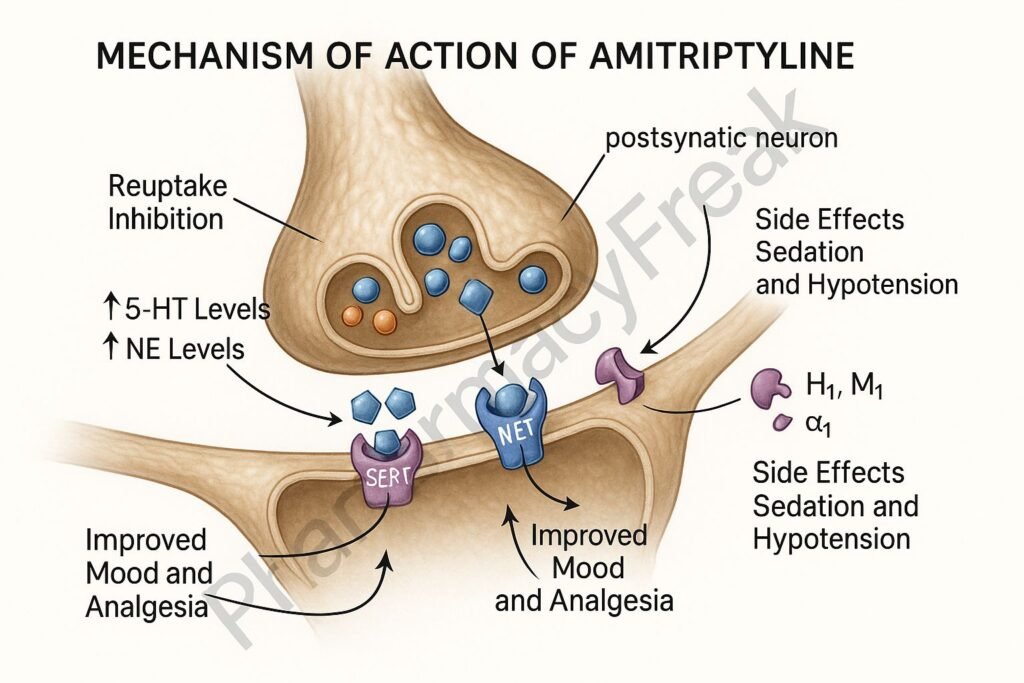
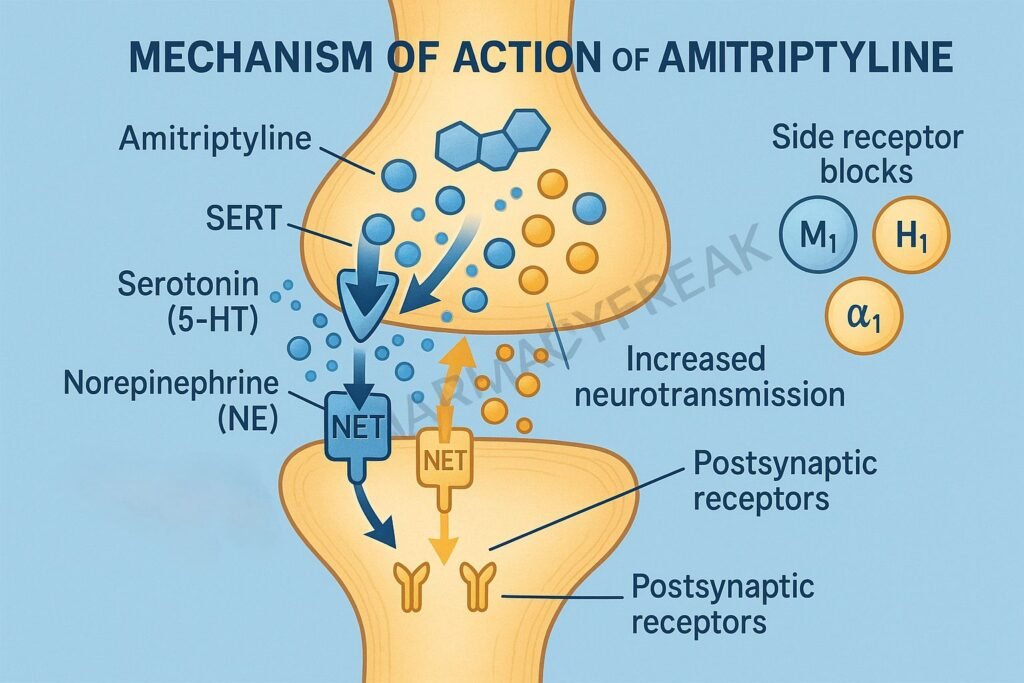
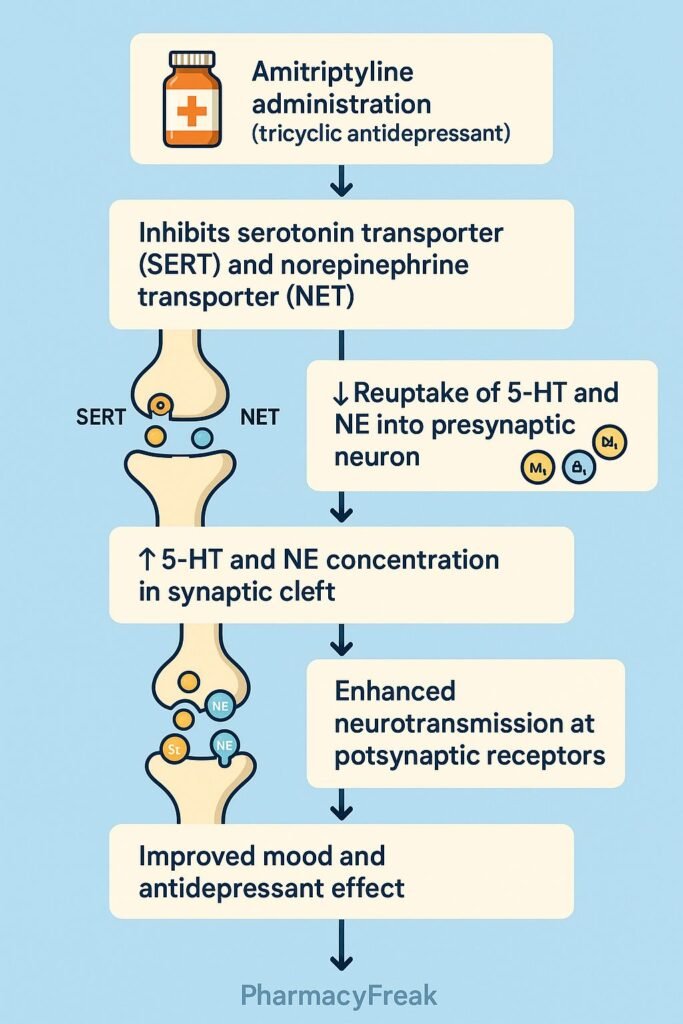
Amitriptyline is a tricyclic antidepressant (TCA) primarily used in the management of major depressive disorder, neuropathic pain, migraine prophylaxis, and insomnia. Mechanism of Action of Amitriptyline involves inhibition of serotonin (5-HT) and norepinephrine (NE) reuptake at presynaptic nerve terminals, thereby increasing their synaptic concentrations. Additionally, it exhibits significant anticholinergic, antihistaminic, and alpha-adrenergic blocking effects, contributing to both its therapeutic and side-effect profiles.
Mechanism of Action (Step-wise)
- Inhibition of Monoamine Reuptake
- Amitriptyline blocks serotonin transporter (SERT) and norepinephrine transporter (NET) in presynaptic neurons.
- This prevents the reuptake of serotonin and norepinephrine, leading to increased neurotransmitter levels in the synaptic cleft.
- The enhanced neurotransmission improves mood, relieves depression, and modulates pain pathways.
- Postsynaptic Receptor Modulation
- Long-term use causes downregulation of postsynaptic β-adrenergic receptors and desensitization of serotonin receptors, which contribute to antidepressant efficacy over time.
- Anticholinergic (Muscarinic Receptor Blockade)
- Amitriptyline blocks muscarinic acetylcholine receptors (M1 subtype), leading to effects such as dry mouth, constipation, and blurred vision.
- Antihistaminic (H1 Receptor Blockade)
- Inhibition of histamine H1 receptors contributes to sedation and weight gain.
- Alpha-Adrenergic Blockade (α1 Receptors)
- Causes orthostatic hypotension and reflex tachycardia due to peripheral vasodilation.
- Sodium Channel Blockade
- At higher concentrations, amitriptyline blocks cardiac Na⁺ channels, potentially causing conduction abnormalities (arrhythmias).
- Overall Effect
- ↑ Serotonin + ↑ Norepinephrine → Antidepressant and analgesic effects
- Anticholinergic + Antihistaminic + Alpha-blockade → Side effects
Pharmacokinetics
- Absorption: Rapid and complete from the gastrointestinal tract.
- Distribution: Highly lipophilic; crosses the blood-brain barrier easily.
- Metabolism: Hepatic via CYP2D6 and CYP2C19 into active metabolite nortriptyline.
- Excretion: Renal (as metabolites).
- Half-life: 15–40 hours.
- Protein binding: >90%.
Clinical Uses
- Major depressive disorder
- Neuropathic pain (postherpetic neuralgia, diabetic neuropathy)
- Migraine prophylaxis
- Chronic tension headache
- Insomnia (due to sedative properties)
- Fibromyalgia (off-label use)
- Irritable bowel syndrome (IBS) — low-dose use for visceral pain modulation
Adverse Effects
- Anticholinergic: Dry mouth, constipation, urinary retention, blurred vision.
- Cardiovascular: Orthostatic hypotension, arrhythmias, QT prolongation.
- CNS: Sedation, confusion (especially in elderly), seizures (in overdose).
- Metabolic: Weight gain, increased appetite.
- Others: Sexual dysfunction, tremor, photosensitivity.
- Toxicity: Overdose can cause cardiac arrhythmias, seizures, and coma — a medical emergency.
Comparative Analysis
| Feature | Amitriptyline | Nortriptyline | Imipramine |
|---|---|---|---|
| Reuptake inhibition | 5-HT and NE | Mainly NE | 5-HT and NE |
| Sedation | High | Moderate | Moderate |
| Anticholinergic effect | Strong | Moderate | Strong |
| Clinical use | Depression, neuropathic pain | Depression, neuropathic pain | Enuresis, depression |
| Active metabolite | Nortriptyline | None | Desipramine |
MCQs
1. Amitriptyline belongs to which class of antidepressants?
a) SSRI
b) SNRI
c) Tricyclic antidepressant
d) MAOI
Answer: c) Tricyclic antidepressant
2. The main mechanism of amitriptyline is:
a) Monoamine oxidase inhibition
b) Reuptake inhibition of serotonin and norepinephrine
c) Dopamine receptor blockade
d) Serotonin receptor antagonism
Answer: b) Reuptake inhibition of serotonin and norepinephrine
3. The major active metabolite of amitriptyline is:
a) Nortriptyline
b) Desipramine
c) Fluoxetine
d) Doxepin
Answer: a) Nortriptyline
4. Amitriptyline causes sedation due to:
a) Dopamine blockade
b) H1 receptor blockade
c) Muscarinic receptor stimulation
d) Alpha receptor activation
Answer: b) H1 receptor blockade
5. Orthostatic hypotension with amitriptyline is due to:
a) Alpha-adrenergic blockade
b) Beta-adrenergic blockade
c) Muscarinic blockade
d) Dopamine antagonism
Answer: a) Alpha-adrenergic blockade
6. Which enzyme primarily metabolizes amitriptyline?
a) CYP3A4
b) CYP2D6
c) CYP2E1
d) CYP1A2
Answer: b) CYP2D6
7. Amitriptyline overdose may cause:
a) Bradycardia and hypothermia
b) Cardiac arrhythmias and seizures
c) Hypertension and tachypnea
d) Respiratory depression only
Answer: b) Cardiac arrhythmias and seizures
8. Which neurotransmitters are increased by amitriptyline?
a) Serotonin and norepinephrine
b) Dopamine and serotonin
c) GABA and glutamate
d) Acetylcholine and histamine
Answer: a) Serotonin and norepinephrine
9. Amitriptyline should be avoided in:
a) Depression
b) Glaucoma and cardiac disease
c) Neuropathic pain
d) Migraine prophylaxis
Answer: b) Glaucoma and cardiac disease
10. Which of the following is NOT a common side effect of amitriptyline?
a) Sedation
b) Dry mouth
c) Urinary retention
d) Hyponatremia
Answer: d) Hyponatremia
FAQs
Q1. What is the mechanism of action of amitriptyline?
It inhibits the reuptake of serotonin and norepinephrine, increasing their synaptic concentrations and improving mood.
Q2. How long does amitriptyline take to work?
It may take 2–4 weeks for full antidepressant effect, though sedative effects occur sooner.
Q3. Can amitriptyline be used for nerve pain?
Yes, it is effective in treating neuropathic pain at lower doses.
Q4. Why does amitriptyline cause drowsiness?
Due to H1 receptor antagonism, leading to central sedation.
Q5. What are the signs of amitriptyline overdose?
Cardiac arrhythmias, convulsions, and coma — requiring immediate medical care.
Q6. Can amitriptyline cause weight gain?
Yes, weight gain is a common side effect due to histamine and serotonin modulation.
References
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics
- Katzung’s Basic and Clinical Pharmacology
- Stahl’s Essential Psychopharmacology
- Harrison’s Principles of Internal Medicine


