Table of Contents
Introduction
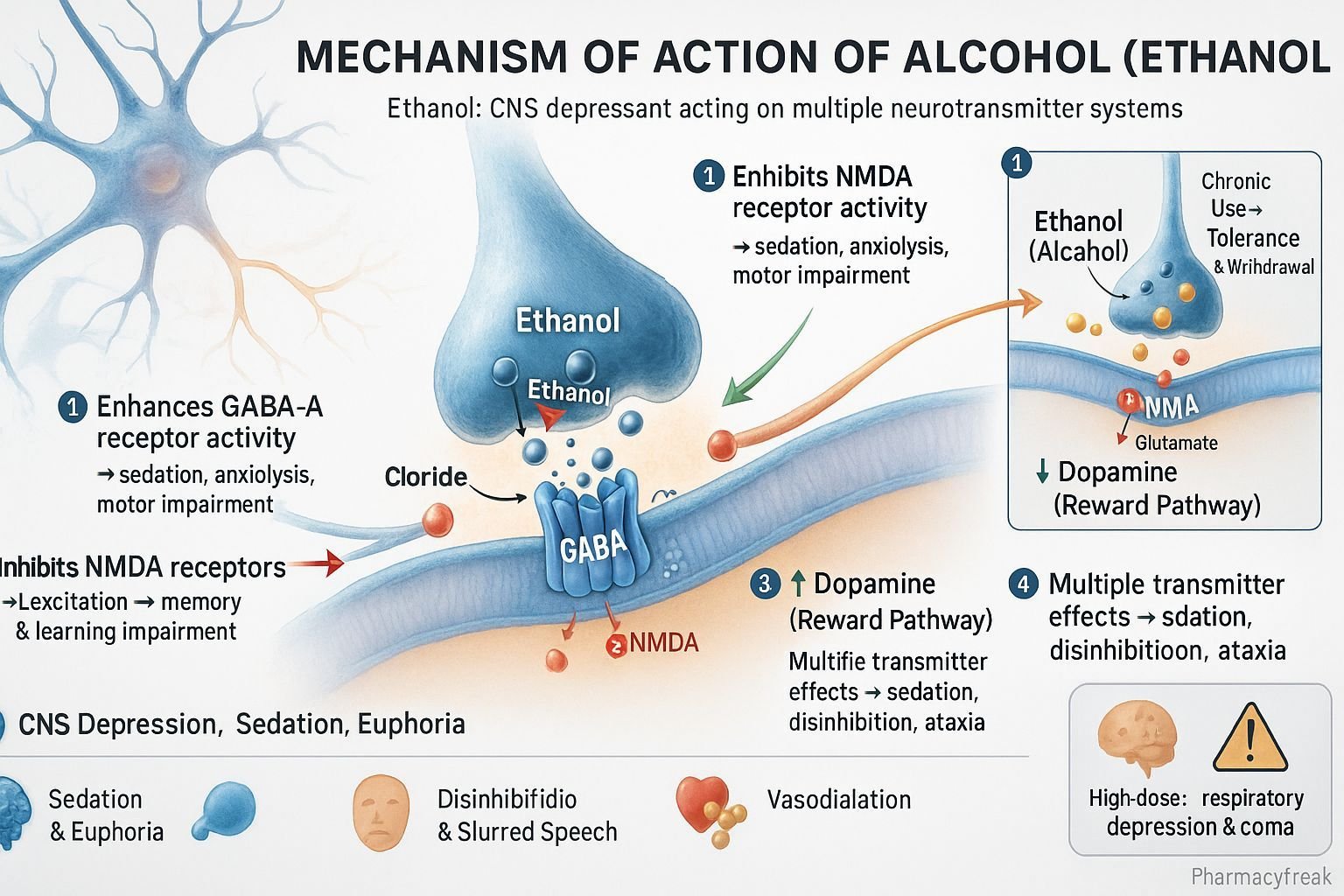
Ethanol, commonly referred to as alcohol, is a psychoactive substance and central nervous system (CNS) depressant with widespread social and clinical significance. Mechanism of Action of Alcohol involves modulation of several neurotransmitter systems—most notably GABA, glutamate, and dopamine—leading to sedation, euphoria, impaired motor coordination, and cognitive effects. Ethanol’s pharmacological effects depend on dose, chronicity of use, and individual susceptibility, influencing both its therapeutic applications (e.g., methanol poisoning) and toxic potential (e.g., dependence and organ damage).
Mechanism of Action (Step-wise)
- Enhancement of GABAergic Transmission
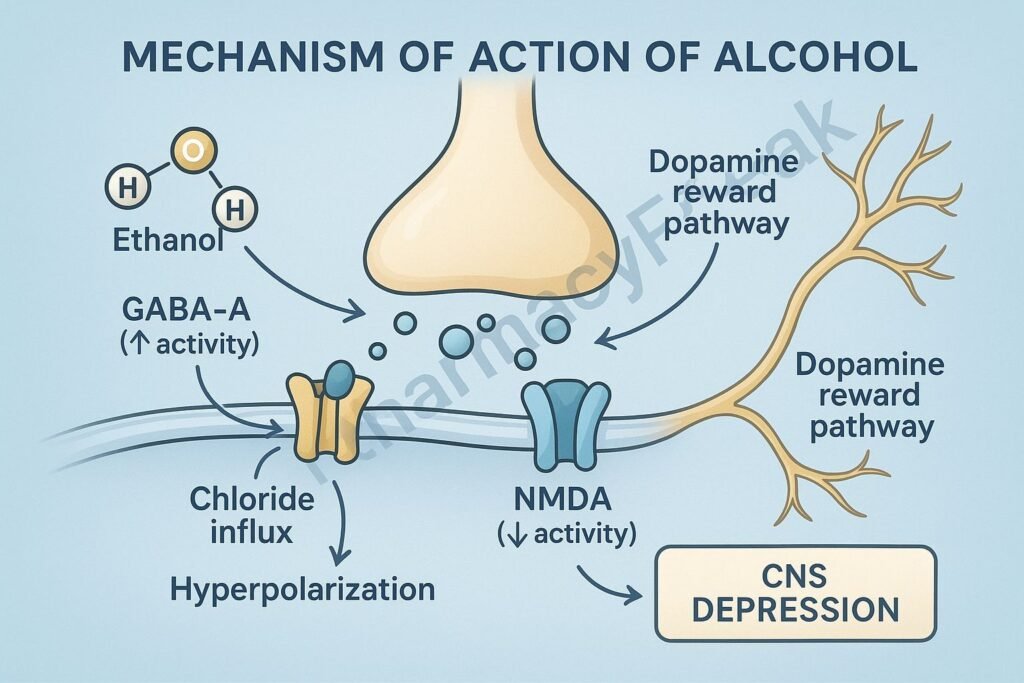
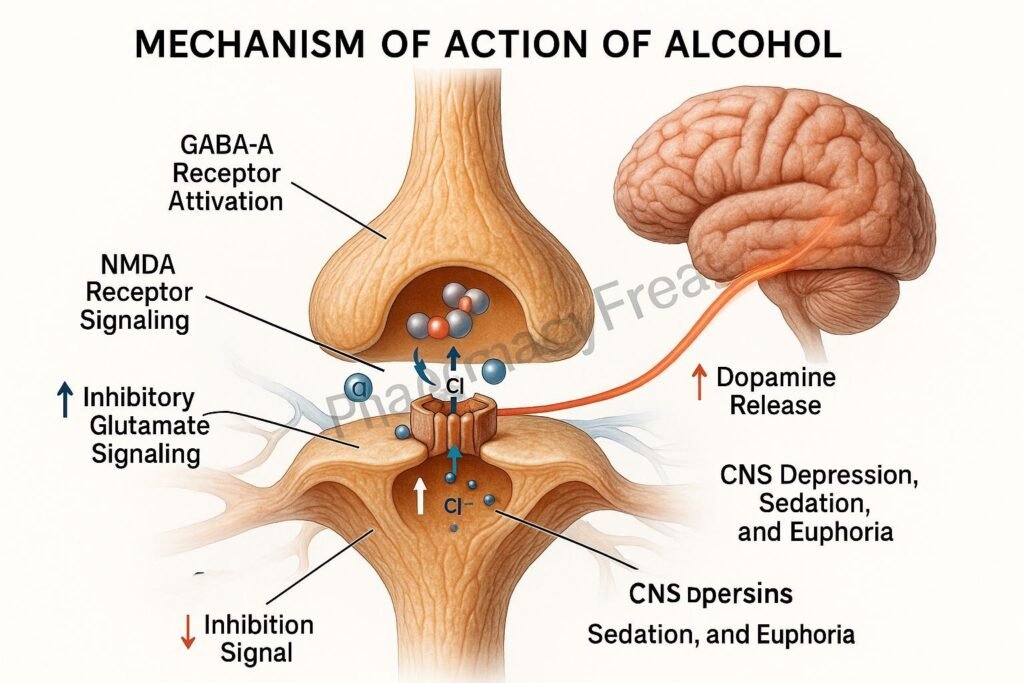
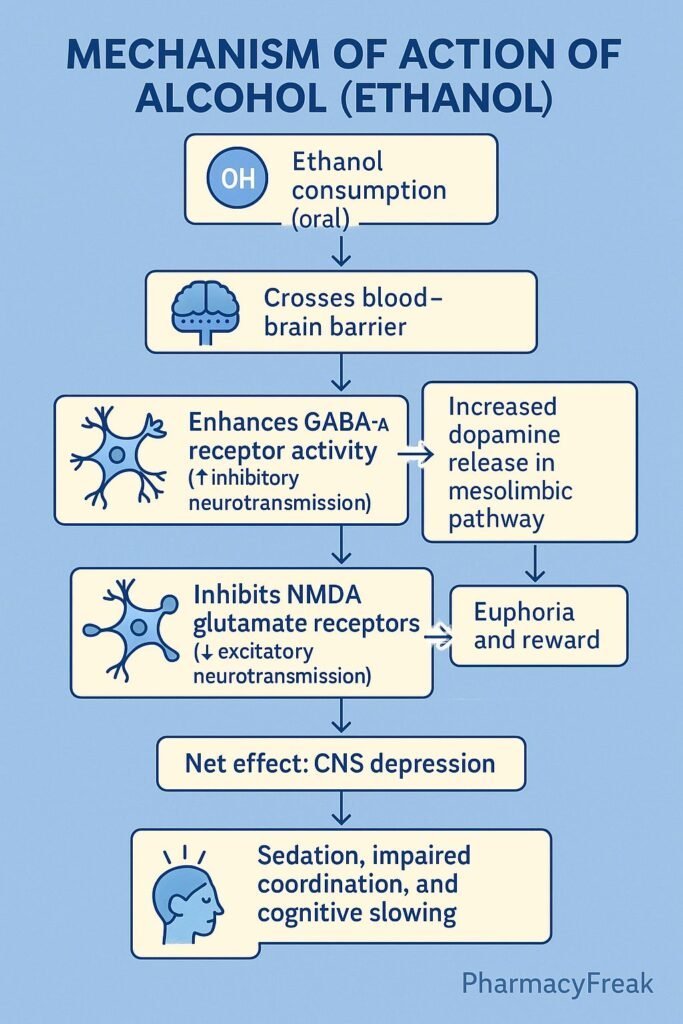
- Alcohol potentiates GABA-A receptor activity, the primary inhibitory neurotransmitter in the CNS.
- Increased chloride ion influx hyperpolarizes neurons, producing sedation, anxiolysis, and motor impairment.
- Inhibition of Glutamatergic Transmission
- Ethanol inhibits NMDA (N-methyl-D-aspartate) receptors, decreasing excitatory neurotransmission.
- This contributes to memory impairment (“blackouts”) and overall CNS depression.
- Dopaminergic System Activation
- Alcohol increases dopamine release in the mesolimbic reward pathway (nucleus accumbens).
- This produces feelings of euphoria and reinforces addictive behaviors.
- Serotonin and Opioid System Modulation
- Enhances serotonin and endogenous opioid activity, influencing mood and reinforcement mechanisms.
- Chronic Adaptation and Tolerance
- Long-term alcohol exposure causes downregulation of GABA receptors and upregulation of NMDA receptors, leading to tolerance and withdrawal symptoms upon cessation.
- Overall Effect
- Acute: Sedation, anxiolysis, euphoria, impaired judgment, loss of coordination.
- Chronic: Dependence, neuroadaptation, liver damage, and neurotoxicity.
Pharmacokinetics
- Absorption: Rapid from stomach and small intestine; rate increased on an empty stomach.
- Distribution: Widely distributed; crosses placenta and blood–brain barrier.
- Metabolism:
- 90–95% metabolized in the liver via alcohol dehydrogenase (ADH) and aldehyde dehydrogenase (ALDH).
- ADH converts ethanol → acetaldehyde → acetate → CO₂ + H₂O.
- CYP2E1 pathway also contributes at higher concentrations (inducible in chronic users).
- Excretion: 2–10% excreted unchanged in urine, sweat, and breath.
- Half-life: Variable; metabolism follows zero-order kinetics (constant rate, independent of concentration).
Clinical Uses
- Antidote in methanol or ethylene glycol poisoning (competes for alcohol dehydrogenase).
- Disinfectant/antiseptic in topical preparations.
- Solvent and preservative in pharmaceuticals.
- Limited medical sedation (historical use only).
Adverse Effects
- Acute: Slurred speech, ataxia, drowsiness, impaired judgment, hypoglycemia.
- Chronic:
- Neurological: Dependence, peripheral neuropathy, Wernicke–Korsakoff syndrome (thiamine deficiency).
- Hepatic: Fatty liver → hepatitis → cirrhosis.
- Cardiovascular: Hypertension, cardiomyopathy.
- Gastrointestinal: Gastritis, pancreatitis.
- Hematologic: Anemia, thrombocytopenia.
- Withdrawal symptoms: Tremors, anxiety, seizures, delirium tremens.
Comparative Analysis
| Feature | Alcohol (Ethanol) | Benzodiazepines | Barbiturates |
|---|---|---|---|
| Main receptor | GABA-A modulation | GABA-A enhancement | GABA-A enhancement |
| Excitatory inhibition | NMDA blockade | Minimal | Minimal |
| Dopamine reward activation | Yes | Mild | Minimal |
| Dependence potential | High | Moderate | High |
| Withdrawal risk | Severe (seizures, DTs) | Moderate | High |
MCQs
1. Alcohol primarily acts as a:
a) CNS stimulant
b) CNS depressant
c) Dopamine antagonist
d) GABA antagonist
Answer: b) CNS depressant
2. Alcohol enhances the activity of which neurotransmitter receptor?
a) NMDA receptor
b) GABA-A receptor
c) Dopamine receptor
d) Serotonin receptor
Answer: b) GABA-A receptor
3. Which neurotransmitter system is inhibited by alcohol?
a) GABA
b) Glutamate (NMDA)
c) Dopamine
d) Serotonin
Answer: b) Glutamate (NMDA)
4. Which enzyme metabolizes ethanol to acetaldehyde?
a) Aldehyde oxidase
b) Alcohol dehydrogenase
c) Monoamine oxidase
d) Catalase
Answer: b) Alcohol dehydrogenase
5. The rate of ethanol metabolism follows:
a) First-order kinetics
b) Zero-order kinetics
c) Second-order kinetics
d) Mixed-order kinetics
Answer: b) Zero-order kinetics
6. Chronic alcohol use induces which hepatic enzyme?
a) CYP1A2
b) CYP2E1
c) CYP3A4
d) CYP2D6
Answer: b) CYP2E1
7. Alcohol withdrawal is due to:
a) Upregulation of GABA receptors
b) Upregulation of NMDA receptors
c) Decrease in serotonin
d) Increase in dopamine
Answer: b) Upregulation of NMDA receptors
8. The antidote for methanol poisoning is:
a) Ethanol
b) Naloxone
c) Atropine
d) Diazepam
Answer: a) Ethanol
9. Wernicke–Korsakoff syndrome is due to deficiency of:
a) Vitamin B₁₂
b) Thiamine (Vitamin B₁)
c) Folic acid
d) Niacin
Answer: b) Thiamine (Vitamin B₁)
10. Which of the following is a major metabolite of ethanol?
a) Formaldehyde
b) Acetaldehyde
c) Acetic acid
d) Methanol
Answer: b) Acetaldehyde
FAQs
Q1. Is alcohol a stimulant or a depressant?
Although it may initially cause stimulation, alcohol is a CNS depressant at all doses.
Q2. Why does alcohol cause euphoria?
It increases dopamine release in the mesolimbic reward pathway.
Q3. Why do chronic alcoholics develop tolerance?
Due to neuroadaptive changes—downregulation of GABA receptors and upregulation of NMDA receptors.
Q4. Can alcohol be used medically?
Yes, in limited cases like methanol or ethylene glycol poisoning and as a disinfectant.
Q5. Why does alcohol withdrawal cause seizures?
Loss of GABA inhibition and NMDA hyperactivity after chronic suppression of CNS excitability.
Q6. How does food affect alcohol absorption?
Food delays gastric emptying, reducing the rate of alcohol absorption.
References
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics
- Katzung’s Basic and Clinical Pharmacology
- Harrison’s Principles of Internal Medicine
- WHO Alcohol Use and Dependence Guidelines

