Table of Contents
Introduction
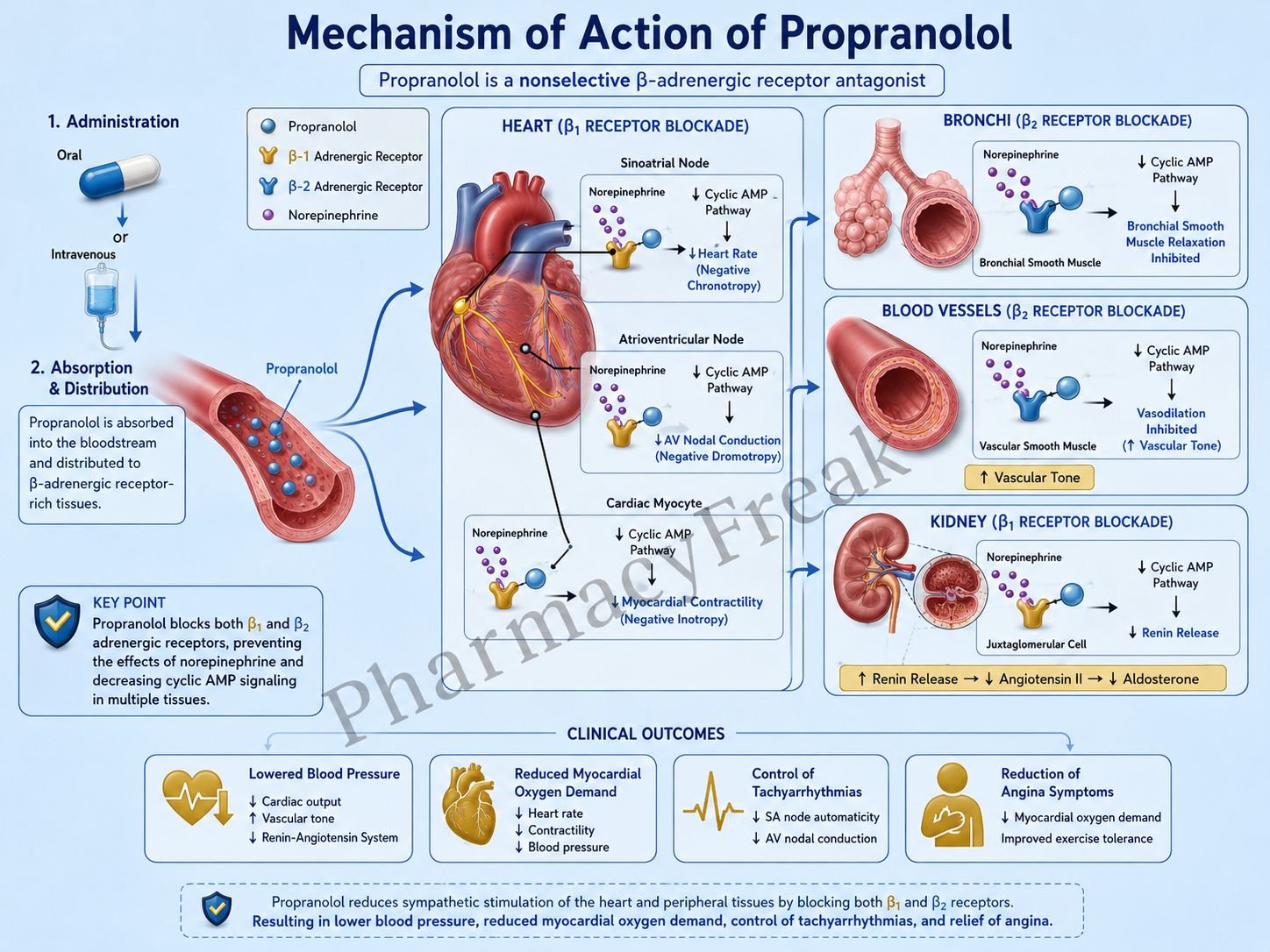
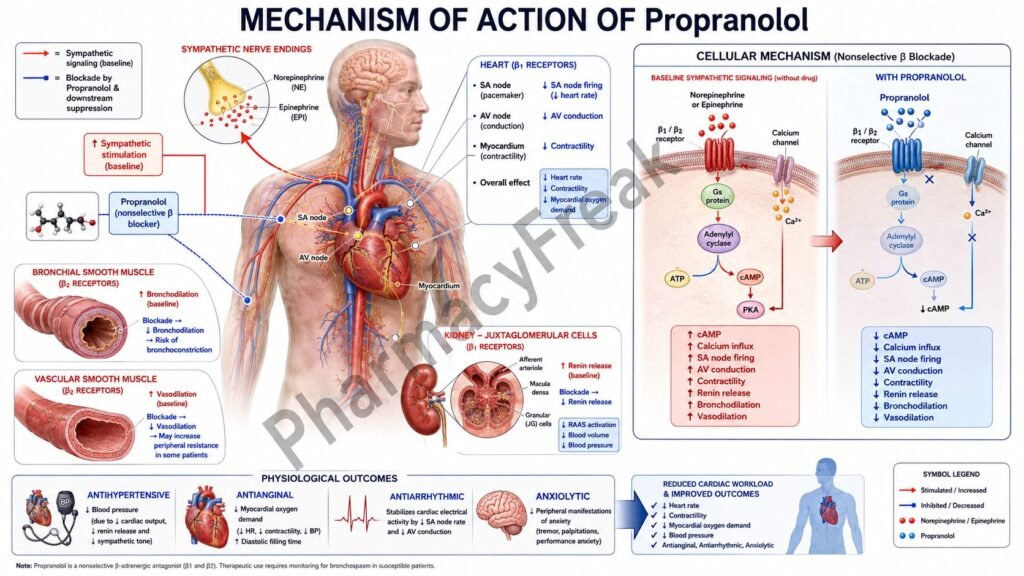
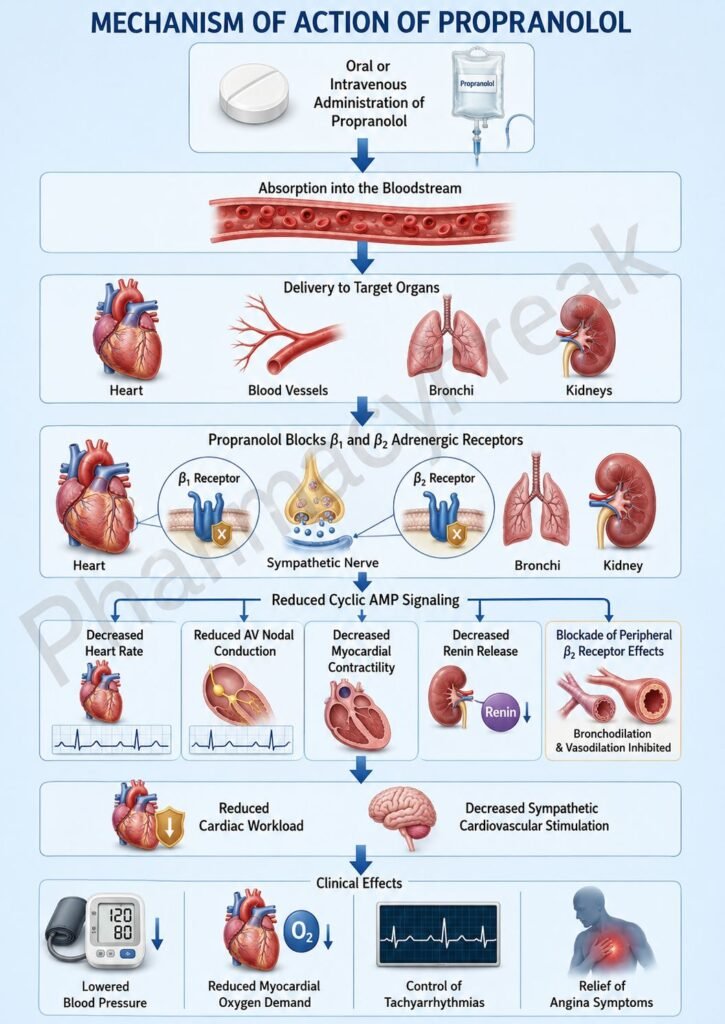
Propranolol is a nonselective β-adrenergic receptor blocker widely used in cardiovascular, neurologic, and endocrine disorders. It blocks both β1 and β2 adrenergic receptors, reducing sympathetic nervous system activity. Propranolol is commonly prescribed in hypertension, angina, arrhythmias, essential tremor, migraine prophylaxis, and hyperthyroidism.
Mechanism of Action (Step-wise)
- Propranolol competitively blocks β1 and β2 adrenergic receptors.
- β receptors are normally stimulated by catecholamines such as epinephrine and norepinephrine.
- β1 receptors in the heart are coupled to Gs proteins.
- Activation of β1 receptors normally increases adenylate cyclase activity and cyclic AMP (cAMP).
- Increased cAMP enhances calcium influx into cardiac cells.
- This increases heart rate, myocardial contractility, and conduction velocity.
- Propranolol blocks β1 receptors, reducing cAMP production.
- Reduced calcium influx decreases heart rate (negative chronotropic effect).
- It also decreases myocardial contractility (negative inotropic effect).
- Cardiac output and myocardial oxygen demand decrease.
- In the kidneys, β1 blockade reduces renin release from juxtaglomerular cells.
- Reduced renin decreases activation of the renin-angiotensin-aldosterone system (RAAS).
- β2 receptor blockade suppresses sympathetic effects in peripheral tissues.
- The overall effect is decreased sympathetic cardiovascular stimulation.
A key exam point is that propranolol is a nonselective β-blocker that reduces heart rate, contractility, and renin release.
Pharmacokinetics
Propranolol is administered orally or intravenously. It undergoes extensive first-pass hepatic metabolism, reducing oral bioavailability. It is highly lipophilic and crosses the blood-brain barrier. Metabolism occurs primarily in the liver, and metabolites are excreted via the kidneys.
Clinical Uses
Propranolol is used in hypertension, angina pectoris, supraventricular tachyarrhythmias, migraine prophylaxis, essential tremor, performance anxiety, and hyperthyroidism. It is also used after myocardial infarction to reduce mortality.
Adverse Effects
Common adverse effects include bradycardia, fatigue, hypotension, and dizziness. Because of β2 blockade, bronchospasm may occur in patients with asthma or COPD. It may also mask symptoms of hypoglycemia in diabetic patients. Abrupt withdrawal can precipitate rebound tachycardia and hypertension.
Comparative Analysis
| Feature | Propranolol | Metoprolol | Atenolol |
|---|---|---|---|
| Receptor selectivity | Nonselective β1 + β2 blocker | β1 selective | β1 selective |
| CNS penetration | High | Moderate | Low |
| Bronchospasm risk | Higher | Lower | Lower |
| Lipid solubility | High | Moderate | Low |
| Main use | Cardiovascular + migraine + tremor | Cardiovascular disease | Hypertension |
| Hyperthyroidism use | Yes | Less common | Less common |
Propranolol differs from metoprolol and atenolol because it blocks both β1 and β2 receptors and readily enters the CNS. Its β2 blockade increases risk of bronchospasm.
MCQs
- Propranolol blocks which receptors?
a) α1 receptors
b) β1 and β2 receptors
c) Muscarinic receptors
d) Dopamine receptors
Answer: b) β1 and β2 receptors
- Propranolol is classified as a:
a) Calcium channel blocker
b) Nonselective β blocker
c) ACE inhibitor
d) Diuretic
Answer: b) Nonselective β blocker
- β1 receptors are mainly located in the:
a) Liver
b) Heart
c) Skin
d) Retina
Answer: b) Heart
- β1 receptor activation normally increases:
a) cAMP
b) Chloride influx
c) Potassium loss
d) Histamine release
Answer: a) cAMP
- Propranolol decreases:
a) Heart rate
b) Blood glucose directly
c) Calcium absorption
d) Histamine release
Answer: a) Heart rate
- Propranolol reduces renin release from the:
a) Liver
b) Juxtaglomerular cells
c) Thyroid gland
d) Pancreas
Answer: b) Juxtaglomerular cells
- A common adverse effect is:
a) Bradycardia
b) Hyperactivity
c) Hypercalcemia
d) Mydriasis
Answer: a) Bradycardia
- β2 blockade by propranolol may cause:
a) Bronchodilation
b) Bronchospasm
c) Hyperglycemia
d) Tachycardia
Answer: b) Bronchospasm
- Propranolol is used for:
a) Migraine prophylaxis
b) Hypercalcemia
c) Glaucoma only
d) Renal failure
Answer: a) Migraine prophylaxis
- Propranolol crosses the blood-brain barrier because it is:
a) Hydrophilic
b) Lipophilic
c) Protein only
d) Polar
Answer: b) Lipophilic
- Abrupt withdrawal of propranolol may cause:
a) Rebound tachycardia
b) Hypoglycemia
c) Hypercalcemia
d) Sedation
Answer: a) Rebound tachycardia
- Compared to metoprolol, propranolol has:
a) β1 selectivity only
b) Higher bronchospasm risk
c) Lower CNS penetration
d) No cardiac effect
Answer: b) Higher bronchospasm risk
FAQs
What is the mechanism of action of propranolol?
It competitively blocks β1 and β2 adrenergic receptors, reducing sympathetic activity.
How does propranolol lower blood pressure?
By decreasing heart rate, cardiac output, and renin release.
Why can propranolol cause bronchospasm?
Because it blocks β2 receptors in bronchial smooth muscle.
What is propranolol commonly used for besides hypertension?
Migraine prophylaxis, essential tremor, and hyperthyroidism.
Why should propranolol not be stopped abruptly?
Because rebound sympathetic activity may occur.
Does propranolol enter the CNS?
Yes, it is highly lipophilic and crosses the blood-brain barrier.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics – Adrenergic Antagonists
https://accessmedicine.mhmedical.com/book.aspx?bookid=3191
Katzung: Basic and Clinical Pharmacology – β-Adrenergic Blocking Drugs
https://accessmedicine.mhmedical.com/content.aspx?bookid=3382
Tripathi: Essentials of Medical Pharmacology – β Blockers
https://www.jaypeedigital.com
Harrison’s Principles of Internal Medicine – Hypertension and Arrhythmias
https://accessmedicine.mhmedical.com

