
Table of Contents
Introduction
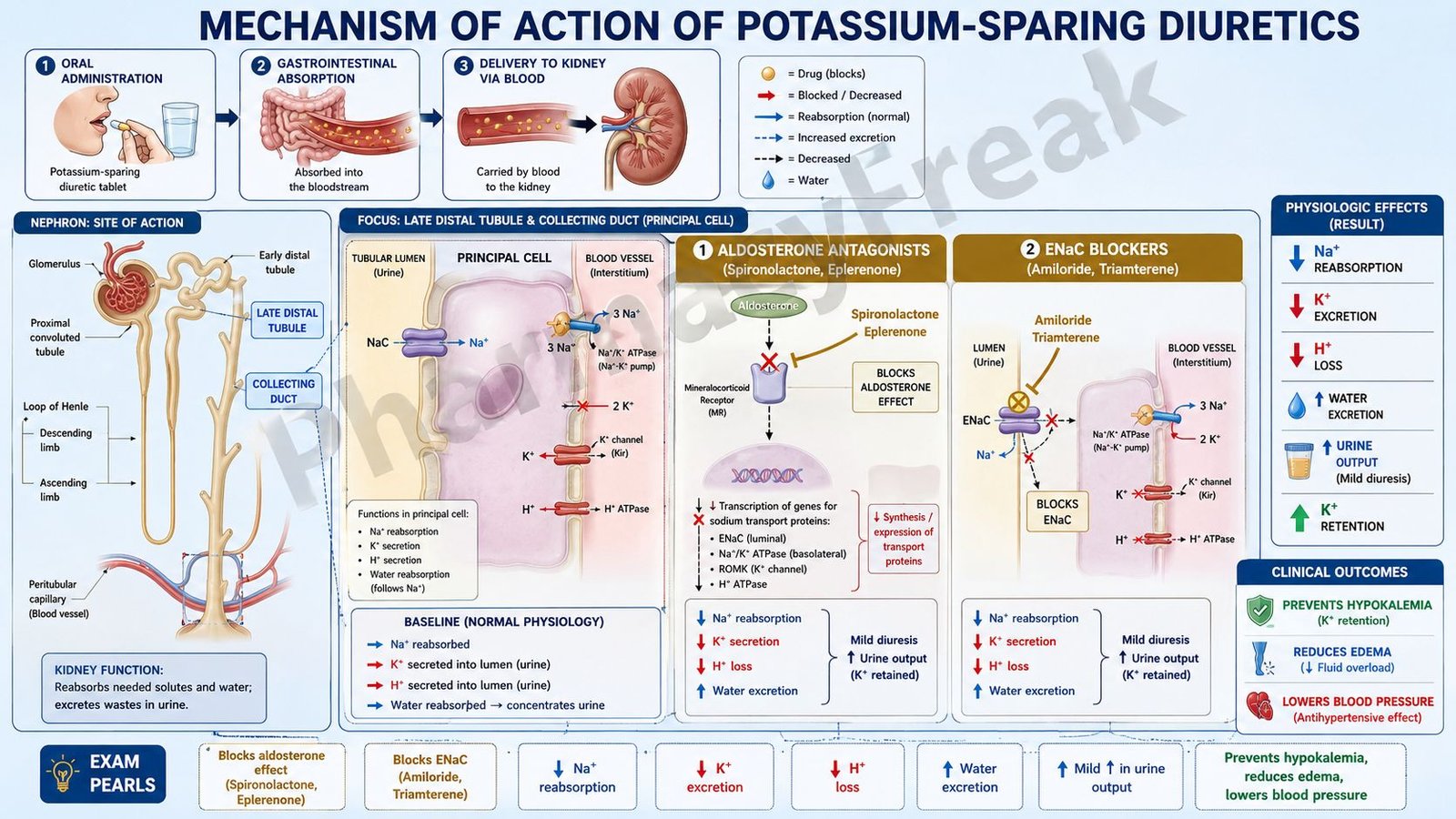
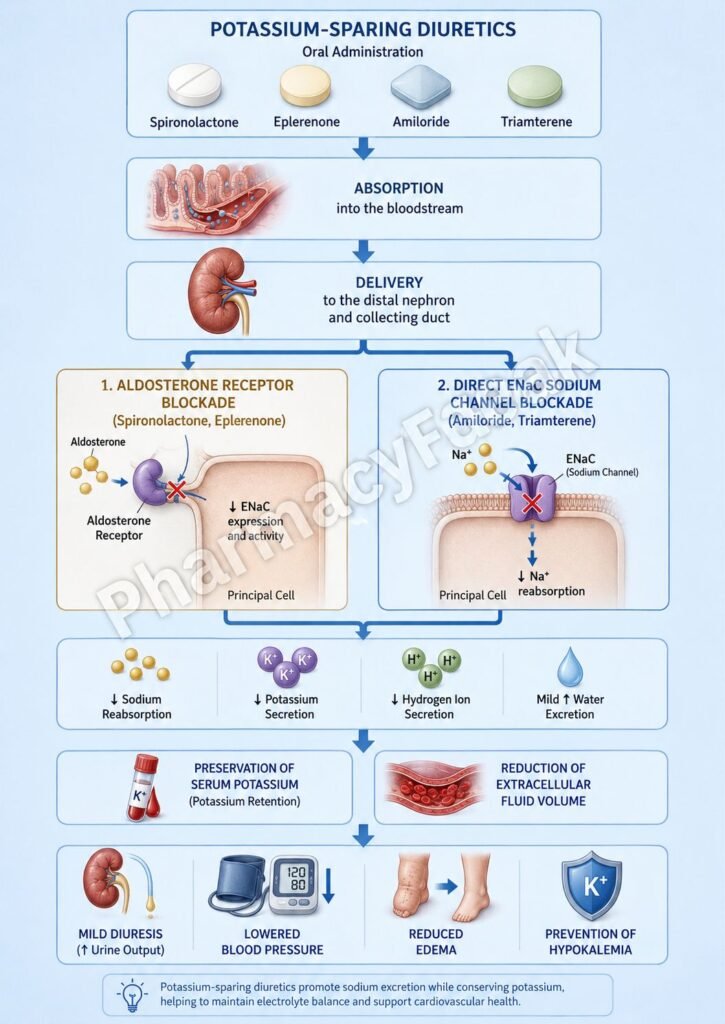
Potassium-sparing diuretics are a group of diuretic drugs that increase sodium and water excretion while conserving potassium. They are mainly used in hypertension, heart failure, hyperaldosteronism, and conditions associated with potassium loss caused by other diuretics. Unlike loop and thiazide diuretics, potassium-sparing diuretics reduce potassium excretion and help prevent hypokalemia.
Mechanism of Action (Step-wise)
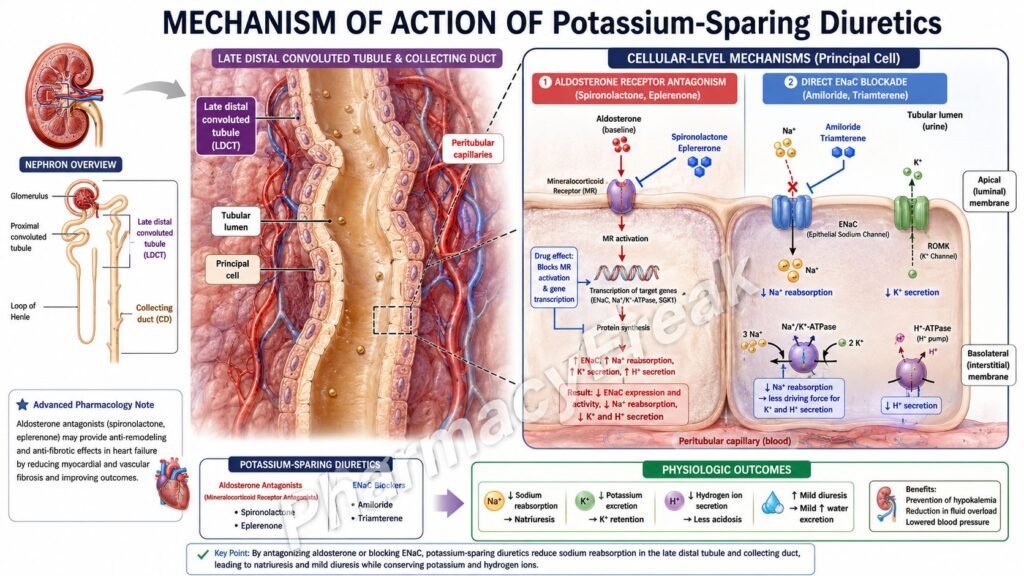
- Potassium-sparing diuretics act in the late distal convoluted tubule and collecting duct of the nephron.
- They are classified into two groups: aldosterone antagonists and epithelial sodium channel (ENaC) blockers.
- Aldosterone antagonists such as spironolactone and eplerenone competitively block mineralocorticoid (aldosterone) receptors.
- Aldosterone normally increases synthesis of ENaC channels and Na⁺/K⁺-ATPase pumps.
- Blocking aldosterone reduces sodium reabsorption and potassium secretion.
- ENaC blockers such as amiloride and triamterene directly inhibit epithelial sodium channels in principal cells.
- Reduced sodium entry into principal cells decreases activity of the Na⁺/K⁺-ATPase.
- This lowers potassium secretion into the tubular lumen.
- Sodium and water excretion increase mildly.
- Potassium retention occurs because less potassium is exchanged for sodium.
- The overall effect is mild diuresis with conservation of potassium.
A key exam point is that potassium-sparing diuretics reduce potassium excretion while promoting mild sodium and water loss.
Pharmacokinetics
Potassium-sparing diuretics are administered orally. Spironolactone is metabolized extensively in the liver to active metabolites. Eplerenone has a shorter duration and greater receptor selectivity. Amiloride and triamterene are excreted mainly by the kidneys. The onset of action of aldosterone antagonists is slower because they alter protein synthesis.
Clinical Uses
Potassium-sparing diuretics are used in hypertension and heart failure, often in combination with loop or thiazide diuretics to prevent hypokalemia. Spironolactone is especially useful in primary hyperaldosteronism, resistant hypertension, and heart failure with reduced ejection fraction. They are also used in ascites associated with liver cirrhosis.
Adverse Effects
The major adverse effect is hyperkalemia, especially in patients with renal impairment or those receiving ACE inhibitors. Spironolactone may cause gynecomastia, impotence, and menstrual irregularities due to antiandrogen effects. Other effects include nausea and dizziness.
Comparative Analysis
| Feature | Potassium-Sparing Diuretics | Loop Diuretics | Thiazide Diuretics |
|---|---|---|---|
| Site of action | Collecting duct | Thick ascending limb | Distal convoluted tubule |
| Potassium effect | Retain potassium | Increase potassium loss | Increase potassium loss |
| Diuretic strength | Mild | Strong | Moderate |
| Main mechanism | Aldosterone blockade or ENaC inhibition | Na⁺-K⁺-2Cl⁻ inhibition | Na⁺-Cl⁻ inhibition |
| Hyperkalemia risk | High | Low | Low |
| Typical use | Prevent hypokalemia | Edema, HF | Hypertension |
Potassium-sparing diuretics differ from loop and thiazide diuretics because they conserve potassium instead of causing potassium wasting. Aldosterone antagonists additionally provide cardiovascular benefits in heart failure.
MCQs
- Potassium-sparing diuretics act mainly in the:
a) Proximal tubule
b) Loop of Henle
c) Collecting duct
d) Glomerulus
Answer: c) Collecting duct
- Spironolactone blocks which receptor?
a) β1 receptor
b) Mineralocorticoid receptor
c) H1 receptor
d) Dopamine receptor
Answer: b) Mineralocorticoid receptor
- Amiloride directly blocks:
a) Na⁺-K⁺-2Cl⁻ transporter
b) ENaC channels
c) Calcium channels
d) H⁺ pumps
Answer: b) ENaC channels
- Potassium-sparing diuretics cause:
a) Potassium loss
b) Potassium retention
c) Calcium loss only
d) Sodium retention
Answer: b) Potassium retention
- The major adverse effect is:
a) Hypokalemia
b) Hyperkalemia
c) Hypercalcemia
d) Hypoglycemia
Answer: b) Hyperkalemia
- Spironolactone is useful in:
a) Hyperaldosteronism
b) Diabetes insipidus
c) Asthma
d) Epilepsy
Answer: a) Hyperaldosteronism
- Aldosterone normally increases:
a) ENaC expression
b) Histamine release
c) Dopamine secretion
d) Insulin production
Answer: a) ENaC expression
- Potassium-sparing diuretics produce which degree of diuresis?
a) Very strong
b) Mild
c) None
d) Extreme
Answer: b) Mild
- Spironolactone may cause:
a) Gynecomastia
b) Ototoxicity
c) Hyperglycemia
d) Bradycardia
Answer: a) Gynecomastia
- ENaC blockers reduce:
a) Sodium entry into principal cells
b) Calcium entry into muscle
c) Histamine release
d) Glucose absorption
Answer: a) Sodium entry into principal cells
- Potassium-sparing diuretics are often combined with:
a) Antifungals
b) Loop diuretics
c) Antivirals
d) Antacids
Answer: b) Loop diuretics
- Compared to loop diuretics, potassium-sparing diuretics:
a) Cause more potassium loss
b) Preserve potassium
c) Have stronger diuresis
d) Cause severe ototoxicity
Answer: b) Preserve potassium
FAQs
What is the mechanism of action of potassium-sparing diuretics?
They reduce sodium reabsorption and potassium secretion in the collecting duct.
Why are they called potassium-sparing?
Because they decrease urinary potassium loss.
What is the difference between spironolactone and amiloride?
Spironolactone blocks aldosterone receptors, while amiloride blocks ENaC channels directly.
What is the major adverse effect?
Hyperkalemia.
Why is spironolactone useful in heart failure?
It blocks harmful effects of aldosterone and improves survival.
Can spironolactone cause hormonal side effects?
Yes, gynecomastia and menstrual irregularities may occur.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics – Diuretics
https://accessmedicine.mhmedical.com/book.aspx?bookid=3191
Katzung: Basic and Clinical Pharmacology – Diuretic Agents
https://accessmedicine.mhmedical.com/content.aspx?bookid=3382
Tripathi: Essentials of Medical Pharmacology – Diuretics
https://www.jaypeedigital.com
Harrison’s Principles of Internal Medicine – Heart Failure and Hypertension
https://accessmedicine.mhmedical.com

