Table of Contents
Introduction
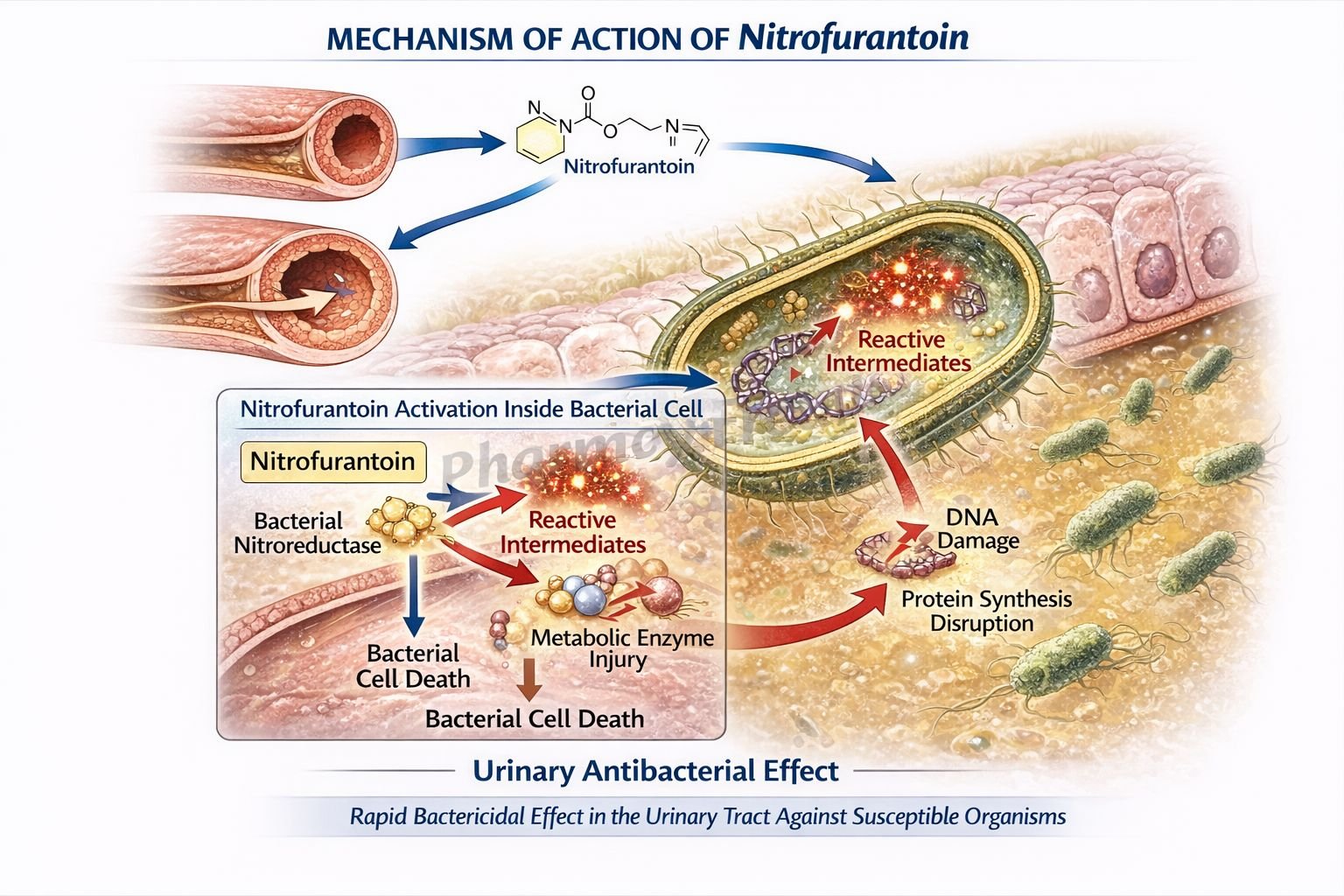
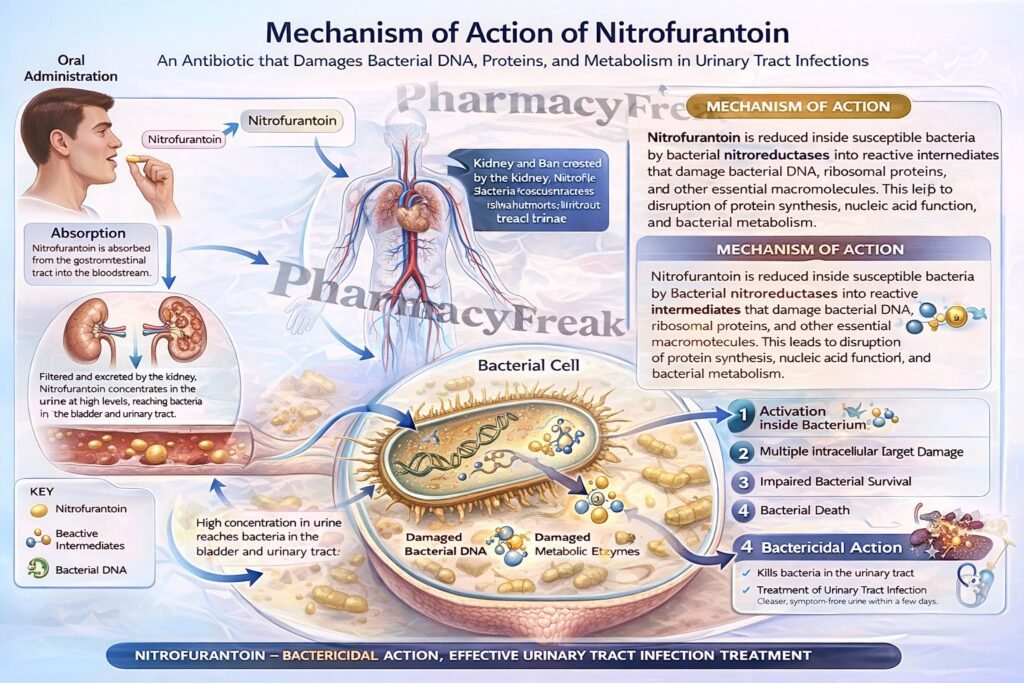
Nitrofurantoin is a nitrofuran antibacterial drug used mainly for uncomplicated lower urinary tract infections. It is especially useful because it achieves therapeutic antibacterial activity in urine and acts through multiple intracellular targets within bacteria. Unlike many antibiotics that inhibit a single enzyme or pathway, nitrofurantoin is reduced inside bacterial cells to highly reactive intermediates that damage several essential bacterial processes. This multi-target action contributes to its antibacterial effect and helps explain the relatively low rate of resistance development. Nitrofurantoin is bactericidal in urine at therapeutic doses.
Mechanism of Action (Step-wise)
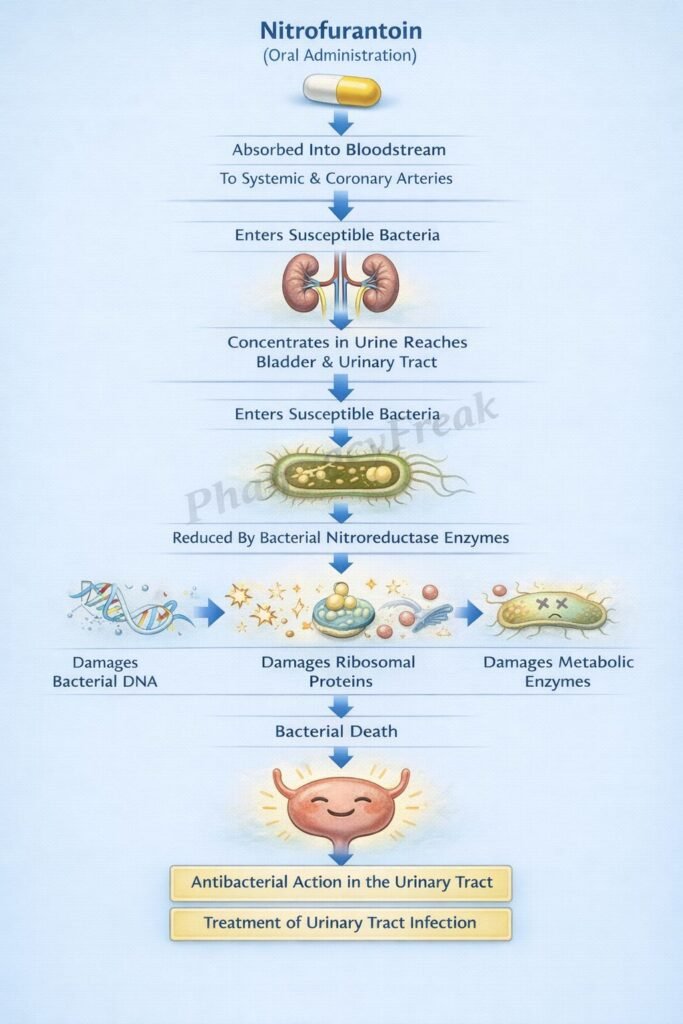
- Nitrofurantoin enters susceptible bacterial cells.
- Inside bacteria, it is reduced by bacterial flavoproteins and nitroreductase systems to reactive intermediates.
- These reactive intermediates inactivate or alter bacterial ribosomal proteins and other macromolecules.
- As a result, multiple vital biochemical pathways are disrupted simultaneously.
- Protein synthesis is inhibited due to ribosomal and enzymatic damage.
- DNA synthesis is impaired.
- RNA synthesis is also inhibited.
- Aerobic energy metabolism is disrupted.
- Cell wall synthesis is additionally affected.
- The combined injury to several essential bacterial functions leads to bacterial death.
- Nitrofurantoin is bactericidal in urine at therapeutic concentrations.
A key exam point is that nitrofurantoin has an unusual multi-target antibacterial mechanism. It does not work like beta-lactams, fluoroquinolones, or sulfonamides, which mainly inhibit one dominant pathway. Instead, its reduced reactive metabolites damage several bacterial macromolecules and metabolic systems at once.
Pharmacokinetics
Nitrofurantoin is administered orally and is rapidly absorbed from the gastrointestinal tract. Macrocrystalline formulations are absorbed more slowly and may improve gastrointestinal tolerability. Food can increase its bioavailability by improving dissolution and absorption. Nitrofurantoin achieves low plasma concentrations but high urinary concentrations, which is why it is mainly useful for lower urinary tract infections rather than systemic infections. It is eliminated largely through the kidneys, where renal excretion is essential for adequate urinary antibacterial levels. Because effective urinary concentration depends on renal function, reduced kidney function can lower efficacy and increase toxicity risk.
Clinical Uses
Nitrofurantoin is primarily used for acute uncomplicated lower urinary tract infections caused by susceptible organisms. It is appropriate for cystitis and is commonly active against organisms such as Escherichia coli and certain other urinary pathogens. It is not suitable for infections requiring high tissue levels, such as renal cortical infection, perinephric abscess, or most systemic infections, because blood and tissue concentrations remain low. This is a classic exam distinction: nitrofurantoin is a urinary antiseptic-like antibacterial used for lower UTI, not pyelonephritis.
Adverse Effects
Common adverse effects include nausea, vomiting, and loss of appetite. Pulmonary toxicity is an important adverse effect and may present as acute hypersensitivity-type pulmonary reactions or chronic pulmonary injury with prolonged use. Peripheral neuropathy can occur, especially in predisposed patients. Hepatic injury is also possible. Hemolytic anemia may occur in patients with glucose-6-phosphate dehydrogenase deficiency. Since renal impairment can increase drug accumulation while reducing urinary efficacy, caution is required in patients with poor renal function.
Comparative Analysis
| Feature | Nitrofurantoin | Trimethoprim-Sulfamethoxazole | Ciprofloxacin |
|---|---|---|---|
| Drug class | Nitrofuran antibacterial | Folate synthesis inhibitor combination | Fluoroquinolone |
| Main mechanism | Reduced to reactive intermediates that damage multiple bacterial macromolecules | Sequential inhibition of folate metabolism | Inhibits DNA gyrase and topoisomerase IV |
| Main site of usefulness | Lower urinary tract | UTI and some systemic infections | UTI and many systemic infections |
| Bactericidal in urine | Yes | Yes | Yes |
| Tissue penetration | Low | Moderate | High |
| Use in pyelonephritis | Poor choice | Possible depending on susceptibility | Common option depending on resistance |
| Resistance pattern | Often relatively preserved for cystitis | Increasing resistance in some regions | Resistance concerns significant |
Nitrofurantoin differs from trimethoprim-sulfamethoxazole and ciprofloxacin because it acts through multiple intracellular reactive intermediates rather than one dominant enzymatic blockade. Its major strength is concentrated urinary activity in lower UTI, while its major limitation is poor tissue penetration for upper urinary or systemic infection.
MCQs
- Nitrofurantoin belongs to which class of antibacterial drugs?
a) Macrolides
b) Nitrofuran antimicrobials
c) Tetracyclines
d) Aminoglycosides
Answer: b) Nitrofuran antimicrobials
- Nitrofurantoin is reduced inside bacterial cells by:
a) Human cytochrome enzymes
b) Bacterial flavoproteins
c) Renal dehydrogenases
d) Lysosomal enzymes
Answer: b) Bacterial flavoproteins
- The active reduced intermediates of nitrofurantoin primarily:
a) Block only cell wall synthesis
b) Block only DNA gyrase
c) Damage multiple bacterial macromolecules
d) Inhibit folate synthesis only
Answer: c) Damage multiple bacterial macromolecules
- Nitrofurantoin inhibits all of the following except:
a) Protein synthesis
b) DNA synthesis
c) RNA synthesis
d) Human steroid synthesis
Answer: d) Human steroid synthesis
- Nitrofurantoin is bactericidal mainly in:
a) Cerebrospinal fluid
b) Plasma
c) Urine
d) Synovial fluid
Answer: c) Urine
- The most appropriate use of nitrofurantoin is:
a) Bacterial meningitis
b) Uncomplicated cystitis
c) Osteomyelitis
d) Bacterial endocarditis
Answer: b) Uncomplicated cystitis
- Nitrofurantoin is a poor choice for pyelonephritis because:
a) It has no antibacterial activity
b) It does not reach adequate tissue levels
c) It is not excreted by kidneys
d) It only acts against Gram-positive organisms
Answer: b) It does not reach adequate tissue levels
- A common gastrointestinal adverse effect of nitrofurantoin is:
a) Constipation
b) Nausea
c) GI bleeding
d) Severe pancreatitis
Answer: b) Nausea
- A serious toxicity associated with long-term nitrofurantoin use is:
a) Ototoxicity
b) Pulmonary toxicity
c) Retinal detachment
d) Adrenal suppression
Answer: b) Pulmonary toxicity
- Nitrofurantoin should be used cautiously in:
a) Hyperthyroidism
b) Renal impairment
c) Peptic ulcer disease
d) Migraine
Answer: b) Renal impairment
- Hemolytic anemia with nitrofurantoin is especially associated with deficiency of:
a) G6PD
b) LDH
c) Pyruvate kinase kinase
d) Carbonic anhydrase
Answer: a) G6PD
- Nitrofurantoin has an unusual mechanism because it:
a) Blocks only ribosomes
b) Is converted to reactive intermediates that affect multiple bacterial processes
c) Inhibits only folate reductase
d) Acts only on fungal membranes
Answer: b) Is converted to reactive intermediates that affect multiple bacterial processes
FAQs
What is the mechanism of action of nitrofurantoin?
Nitrofurantoin is reduced by bacterial flavoproteins to reactive intermediates that damage ribosomal proteins and other macromolecules, thereby inhibiting protein synthesis, DNA synthesis, RNA synthesis, energy metabolism, and cell wall synthesis.
Why is nitrofurantoin mainly used for UTI?
Because it reaches high antibacterial concentrations in urine but relatively low concentrations in blood and tissues.
Is nitrofurantoin bactericidal or bacteriostatic?
At therapeutic urinary concentrations, it is bactericidal in urine.
Why is nitrofurantoin not preferred for pyelonephritis?
It does not achieve adequate renal parenchymal or systemic tissue concentrations.
What is a major long-term toxicity of nitrofurantoin?
Pulmonary toxicity is one of the most important long-term adverse effects.
Why can food improve nitrofurantoin absorption?
Food may improve dissolution and increase bioavailability, especially for some formulations.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics – Antibacterial Drugs
Katzung: Basic and Clinical Pharmacology – Antimicrobial Agents
Tripathi: Essentials of Medical Pharmacology – Antimicrobial Drugs
Harrison’s Principles of Internal Medicine – Urinary Tract Infections

