Table of Contents
Introduction
Fluoxetine is a selective serotonin reuptake inhibitor (SSRI) widely used in the treatment of depressive and anxiety disorders. It was the first SSRI introduced into clinical practice and remains highly relevant due to its long half-life, activating profile, and extensive exam coverage. Fluoxetine is particularly important in pharmacology examinations because of its mechanism at the serotonin transporter, delayed onset of action, and prominent drug–drug interactions.
Mechanism of Action (Step-wise)
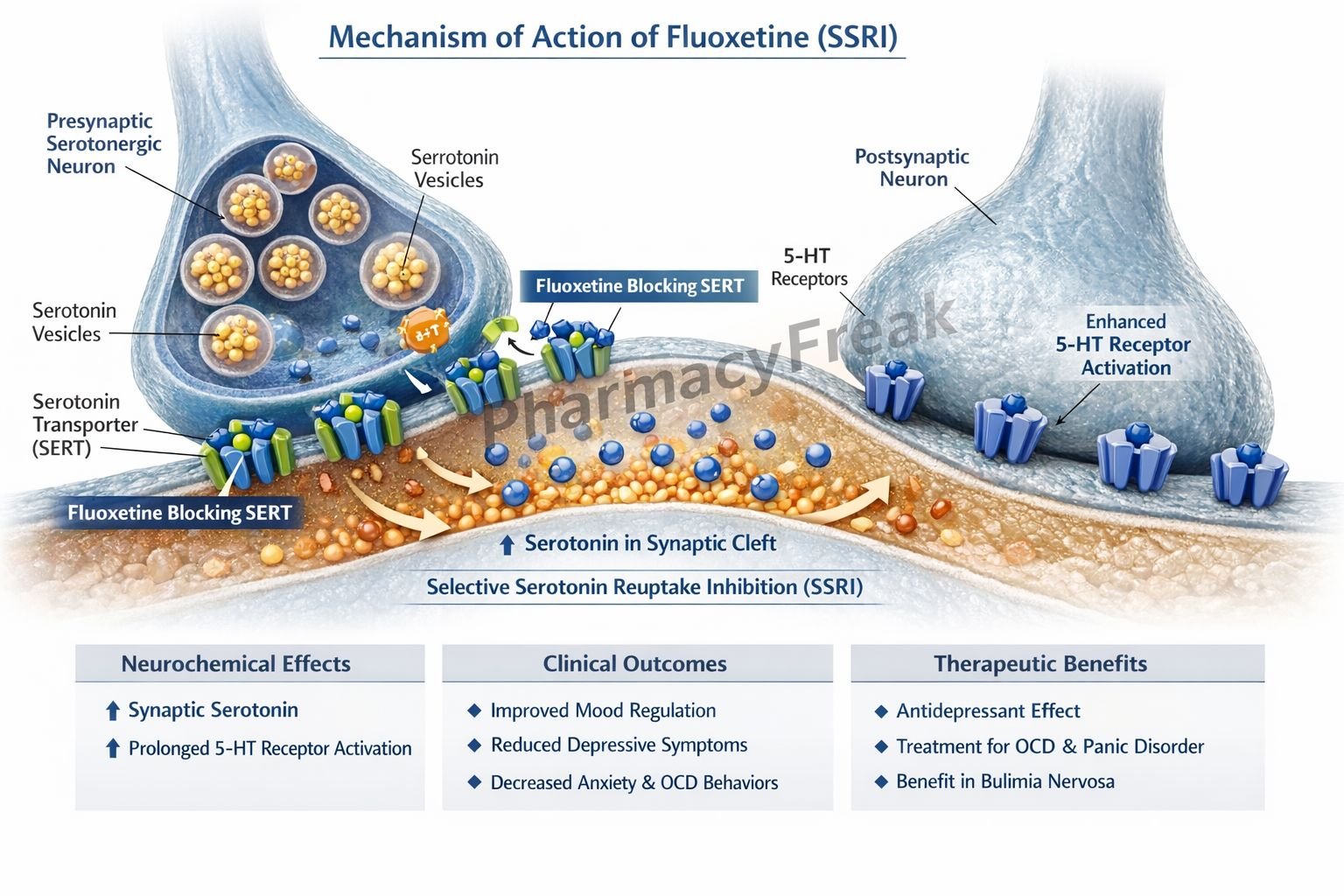
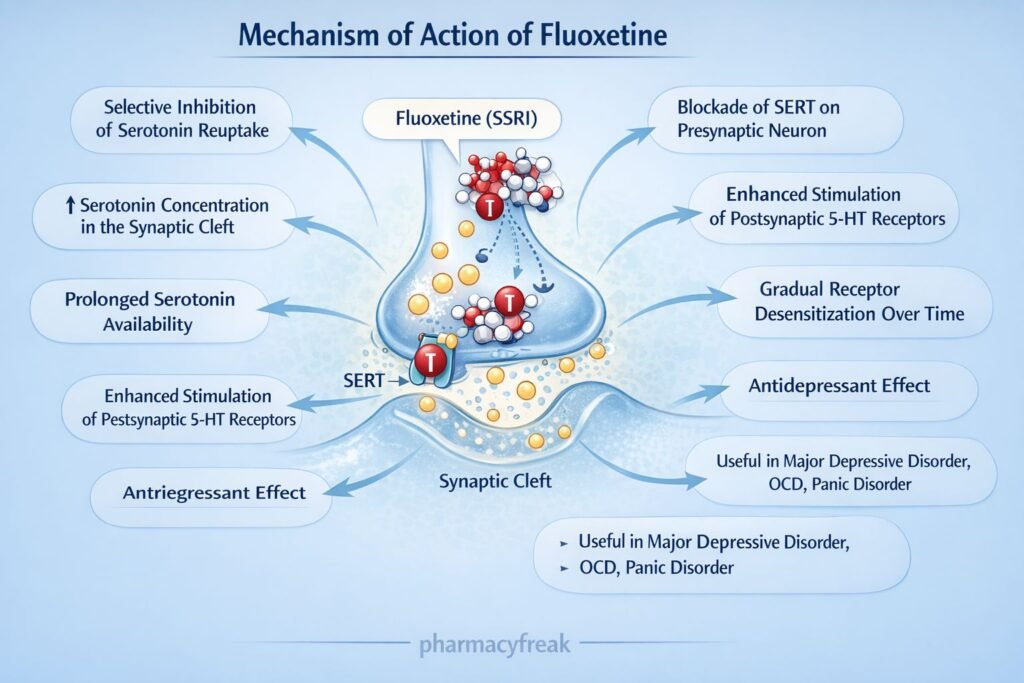
Fluoxetine enhances serotonergic neurotransmission by selectively inhibiting serotonin reuptake.
Step 1: Action at serotonergic synapses
Fluoxetine acts on serotonergic neurons in the brain, especially in the limbic system and cerebral cortex.
Step 2: Inhibition of serotonin transporter (SERT)
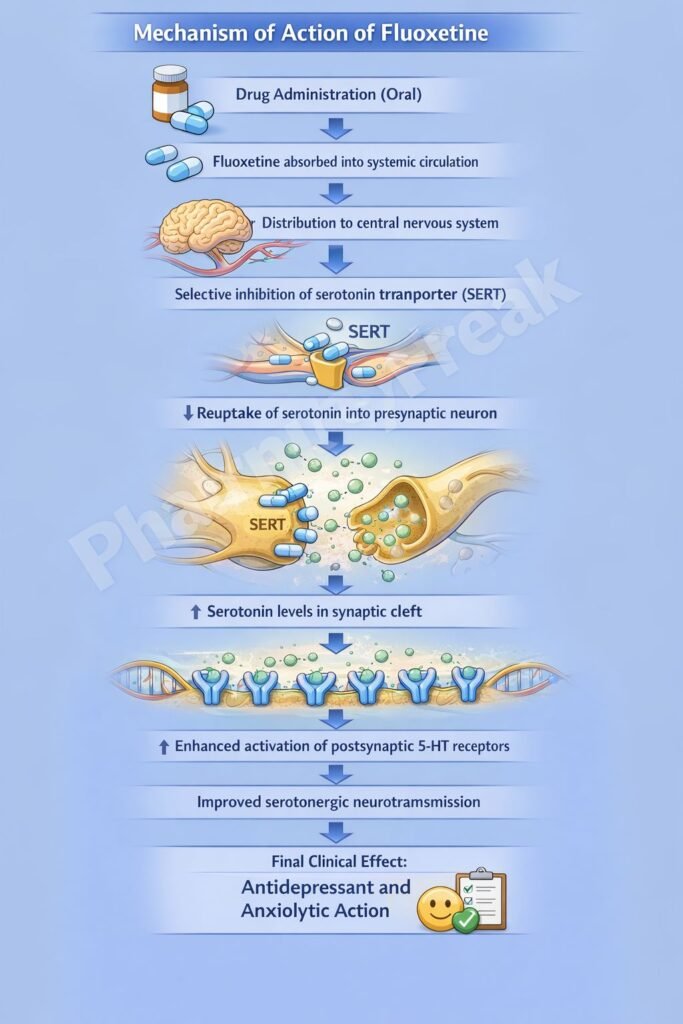
It selectively inhibits the serotonin transporter (SERT) located on the presynaptic neuronal membrane.
Step 3: Reduced serotonin reuptake
Blockade of SERT prevents reabsorption of serotonin (5-HT) into the presynaptic neuron.
Step 4: Increased synaptic serotonin levels
Serotonin accumulates in the synaptic cleft, leading to enhanced stimulation of postsynaptic 5-HT receptors.
Step 5: Long-term adaptive neuronal changes
Chronic use causes downregulation of presynaptic 5-HT₁ autoreceptors and altered gene expression, resulting in sustained antidepressant and anxiolytic effects.
Exam pearl:
Fluoxetine has no significant effect on norepinephrine or dopamine reuptake at therapeutic doses.
Pharmacokinetics
- Route of administration: Oral
- Bioavailability: ~70%
- Protein binding: ~94%
- Distribution: Extensive CNS penetration
- Metabolism: Hepatic (CYP2D6 inhibition)
- Active metabolite: Norfluoxetine
- Half-life:
- Fluoxetine: 2–4 days
- Norfluoxetine: 7–15 days
- Excretion: Urine (metabolites)
- Washout period: Long (important before starting MAOIs)
Clinical Uses
- Major depressive disorder
- Obsessive–compulsive disorder (OCD)
- Bulimia nervosa
- Panic disorder
- Premenstrual dysphoric disorder (PMDD)
- Generalized anxiety disorder (off-label)
Fluoxetine is often preferred in patients with hypersomnia and low energy due to its activating effect.
Adverse Effects
Common:
- Nausea
- Insomnia
- Anxiety or agitation
- Headache
Sexual dysfunction:
- Decreased libido
- Delayed ejaculation
- Anorgasmia
Central nervous system:
- Tremor
- Akathisia (rare)
Serious:
- Serotonin syndrome
- Increased suicidal ideation (early therapy, young patients)
Drug interactions:
- Potent CYP2D6 inhibition
Comparative Analysis
Fluoxetine vs Sertraline vs Paroxetine
| Feature | Fluoxetine | Sertraline | Paroxetine |
|---|---|---|---|
| Half-life | Very long | Moderate | Short |
| Active metabolite | Yes | No | No |
| CYP inhibition | Strong | Mild | Strong |
| Sedation | Minimal | Minimal | Marked |
| Withdrawal symptoms | Rare | Moderate | Common |
Explanation:
Fluoxetine’s long half-life and active metabolite reduce withdrawal symptoms but increase the risk of drug interactions. Paroxetine is more sedating and has prominent discontinuation symptoms.
MCQs
- Fluoxetine primarily inhibits:
a) Dopamine transporter
b) Norepinephrine transporter
c) Serotonin transporter
d) Monoamine oxidase
Answer: c) Serotonin transporter
- Active metabolite of fluoxetine is:
a) Desipramine
b) Norfluoxetine
c) Sertraline
d) Paroxetine
Answer: b) Norfluoxetine
- Fluoxetine has a long washout period because of:
a) High protein binding
b) Renal excretion
c) Active metabolite
d) Poor metabolism
Answer: c) Active metabolite
- Fluoxetine is especially useful in:
a) Hypersomnia
b) Depression with low energy
c) Severe anxiety
d) Bipolar disorder
Answer: b) Depression with low energy
- Enzyme strongly inhibited by fluoxetine is:
a) CYP3A4
b) CYP2C9
c) CYP2D6
d) MAO-A
Answer: c) CYP2D6
- Fluoxetine causes antidepressant effect mainly by increasing:
a) Dopamine
b) GABA
c) Serotonin
d) Acetylcholine
Answer: c) Serotonin
- Sexual dysfunction with fluoxetine is due to:
a) Dopamine blockade
b) Excess serotonin
c) Anticholinergic effect
d) α-blockade
Answer: b) Excess serotonin
- Fluoxetine discontinuation syndrome is:
a) Severe
b) Moderate
c) Mild
d) Absent
Answer: c) Mild
- Risk of serotonin syndrome increases when combined with:
a) NSAIDs
b) Tricyclic antidepressants
c) MAO inhibitors
d) Benzodiazepines
Answer: c) MAO inhibitors
- Fluoxetine is FDA-approved for:
a) Bulimia nervosa
b) Bipolar disorder
c) Schizophrenia
d) ADHD
Answer: a) Bulimia nervosa
FAQs
1. Why does fluoxetine take weeks to work?
Due to gradual receptor and neuronal adaptations.
2. Does fluoxetine cause weight gain?
It is generally weight-neutral or causes mild weight loss initially.
3. Why is fluoxetine safer for discontinuation?
Because of its long half-life and active metabolite.
4. Can fluoxetine be used in OCD?
Yes, it is FDA-approved for OCD.
5. Why is fluoxetine avoided with MAOIs?
Risk of serotonin syndrome due to excessive serotonergic activity.
References
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics
https://accesspharmacy.mhmedical.com - Katzung BG. Basic and Clinical Pharmacology
https://accessmedicine.mhmedical.com - Tripathi KD. Essentials of Medical Pharmacology
- Harrison’s Principles of Internal Medicine
https://accessmedicine.mhmedical.com


