Table of Contents
Introduction
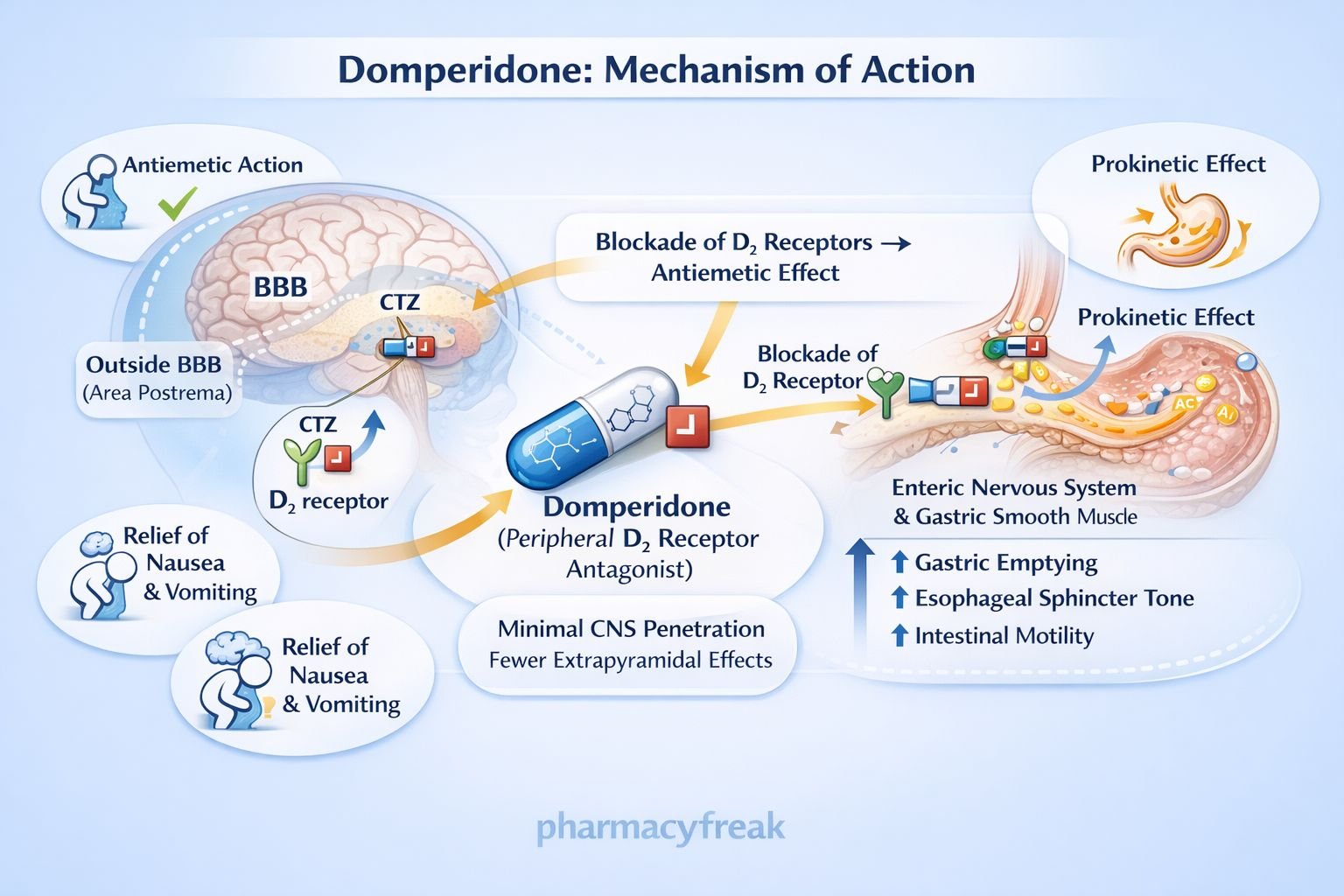
Domperidone is a peripherally selective dopamine D₂ receptor antagonist used primarily as a prokinetic and antiemetic agent. It enhances gastrointestinal motility and suppresses nausea and vomiting without significant central nervous system effects because of its poor penetration across the blood–brain barrier. Domperidone is a high-yield drug in pharmacology, gastroenterology, and clinical examinations due to its dopamine antagonism–based mechanism and favorable CNS safety profile compared with metoclopramide.
Mechanism of Action (Step-wise)
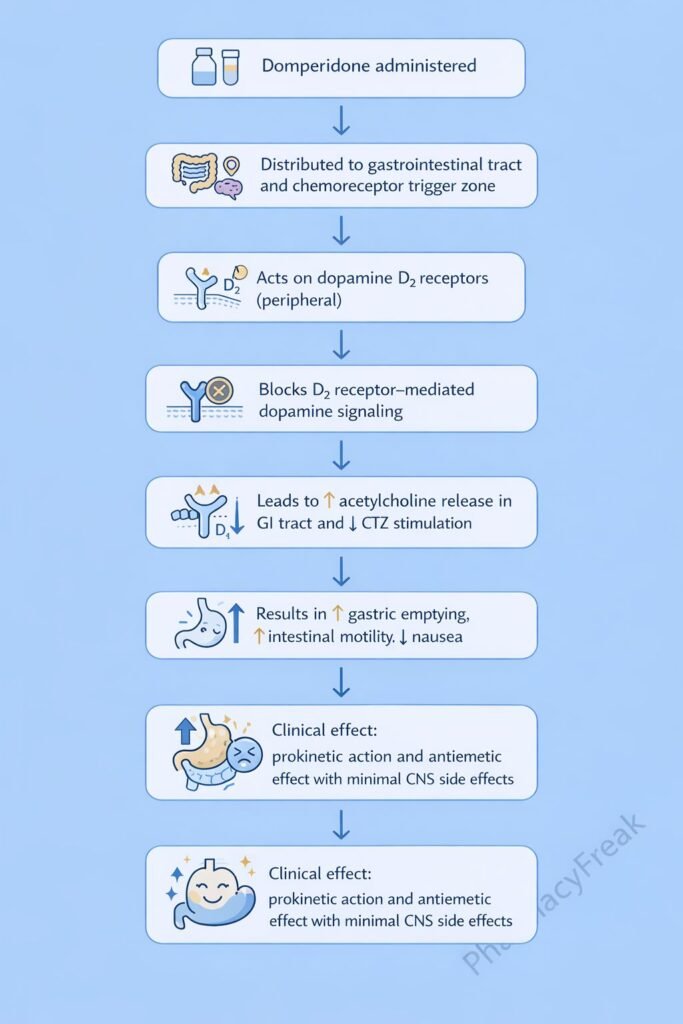
Domperidone improves gastric motility and controls emesis by blocking dopamine D₂ receptors in the gastrointestinal tract and chemoreceptor trigger zone.
Step-wise mechanism:
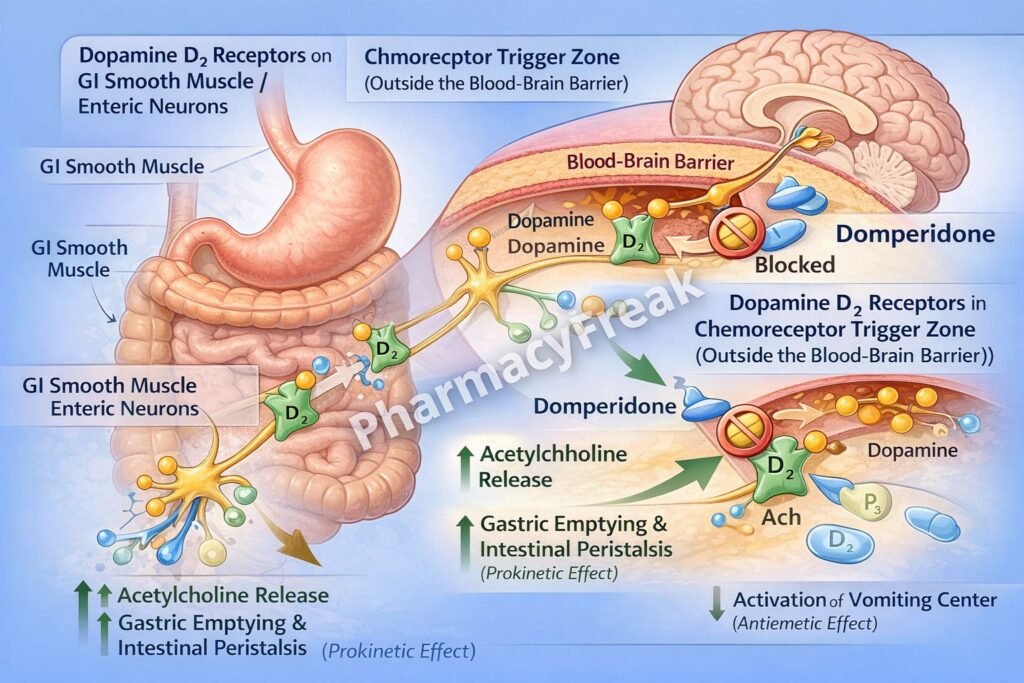
- Physiologic Role of Dopamine in the GI Tract
Dopamine inhibits gastrointestinal motility by acting on dopamine D₂ receptors in the enteric nervous system. - Dopamine D₂ Receptor Antagonism
Domperidone competitively blocks D₂ receptors located on presynaptic enteric neurons. - Disinhibition of Acetylcholine Release
Blocking D₂ receptors removes dopamine-mediated inhibition, increasing acetylcholine release. - Enhanced GI Smooth Muscle Contraction
Increased acetylcholine stimulates muscarinic receptors on GI smooth muscle. - Increased Gastric and Intestinal Motility
This leads to:- Increased lower esophageal sphincter (LES) tone
- Accelerated gastric emptying
- Improved intestinal peristalsis
- Antiemetic Action (Peripheral CTZ Blockade)
Domperidone blocks D₂ receptors in the chemoreceptor trigger zone (outside the BBB), reducing nausea and vomiting. - Minimal Central Effects
Poor CNS penetration results in negligible extrapyramidal side effects.
Pharmacokinetics
- Absorption: Moderate oral absorption
- Bioavailability: Low–moderate due to first-pass metabolism
- Distribution: Limited CNS penetration
- Metabolism: Hepatic metabolism (CYP3A4)
- Elimination: Fecal and renal excretion
- Half-life: Approximately 7–9 hours
Clinical Uses
Domperidone is used in disorders of gastric motility and nausea:
- Gastroesophageal reflux disease (GERD)
- Functional dyspepsia
- Diabetic gastroparesis
- Nausea and vomiting (drug-induced, postoperative)
- Parkinson disease–related nausea (adjunct)
- Lactation enhancement (off-label, due to prolactin increase)
Adverse Effects
Adverse effects are generally mild and predictable:
- Endocrine:
- Hyperprolactinemia
- Galactorrhea
- Gynecomastia
- Cardiac:
- QT interval prolongation
- Ventricular arrhythmias (high dose or IV use)
- Gastrointestinal:
- Dry mouth
- Abdominal cramps
Domperidone should be used cautiously in patients with cardiac disease.
Comparative Analysis (must include a table + explanation)
Comparison of Prokinetic and Antiemetic Drugs
| Feature | Domperidone | Metoclopramide | Ondansetron |
|---|---|---|---|
| Primary mechanism | D₂ receptor blockade (peripheral) | D₂ blockade + 5-HT₄ agonism | 5-HT₃ antagonism |
| CNS penetration | Minimal | Significant | Minimal |
| EPS risk | Rare | Common | None |
| Prokinetic effect | Yes | Yes | No |
| QT prolongation | Possible | Rare | Possible |
Explanation:
Domperidone provides effective prokinetic and antiemetic action with minimal extrapyramidal effects due to poor CNS penetration. Metoclopramide is more potent centrally but carries a higher EPS risk, while ondansetron lacks prokinetic activity.
MCQs (10–15)
- Domperidone primarily blocks which receptor?
a) Serotonin 5-HT₃
b) Dopamine D₂
c) Histamine H₁
d) Muscarinic M₃
Answer: b) Dopamine D₂
- Domperidone increases GI motility by increasing release of:
a) Dopamine
b) Serotonin
c) Acetylcholine
d) GABA
Answer: c) Acetylcholine
- Domperidone differs from metoclopramide because it:
a) Is centrally acting
b) Has strong EPS risk
c) Does not cross BBB significantly
d) Has no antiemetic effect
Answer: c) Does not cross BBB significantly
- Domperidone increases which GI parameter?
a) Gastric acid secretion
b) Lower esophageal sphincter tone
c) Intestinal secretion
d) Colonic water absorption
Answer: b) Lower esophageal sphincter tone
- Domperidone is most useful in:
a) Acute diarrhea
b) Gastroparesis
c) Intestinal obstruction
d) Peptic ulcer bleeding
Answer: b) Gastroparesis
- A major endocrine adverse effect of domperidone is:
a) Hypothyroidism
b) Hyperprolactinemia
c) Hypercortisolism
d) Diabetes mellitus
Answer: b) Hyperprolactinemia
- Domperidone produces antiemetic action by blocking D₂ receptors in the:
a) Vomiting center
b) Vestibular nucleus
c) Chemoreceptor trigger zone
d) Cerebral cortex
Answer: c) Chemoreceptor trigger zone
- Domperidone should be used cautiously due to risk of:
a) Nephrotoxicity
b) Hepatic failure
c) QT prolongation
d) Hypoglycemia
Answer: c) QT prolongation
- Domperidone has minimal extrapyramidal effects because it:
a) Is weak
b) Is rapidly metabolized
c) Poorly enters the CNS
d) Blocks serotonin receptors
Answer: c) Poorly enters the CNS
- Domperidone is metabolized mainly by:
a) CYP2C9
b) CYP2D6
c) CYP3A4
d) MAO
Answer: c) CYP3A4
FAQs (minimum 5)
- What is the primary mechanism of domperidone?
Peripheral dopamine D₂ receptor antagonism increasing GI motility. - Why does domperidone have fewer CNS side effects?
Because it poorly crosses the blood–brain barrier. - Is domperidone a prokinetic drug?
Yes, it enhances gastric emptying and intestinal peristalsis. - Why can domperidone increase prolactin levels?
Due to dopamine blockade in the pituitary. - Is domperidone safer than metoclopramide?
It has fewer extrapyramidal effects but carries a QT-prolongation risk. - Can domperidone be used for GERD?
Yes, as an adjunct due to increased LES tone and gastric emptying.
References
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics
https://accessmedicine.mhmedical.com - Katzung BG. Basic and Clinical Pharmacology
https://accessmedicine.mhmedical.com - Tripathi KD. Essentials of Medical Pharmacology
https://www.jaypeebrothers.com - Harrison’s Principles of Internal Medicine
https://accessmedicine.mhmedical.com


