Table of Contents
Introduction
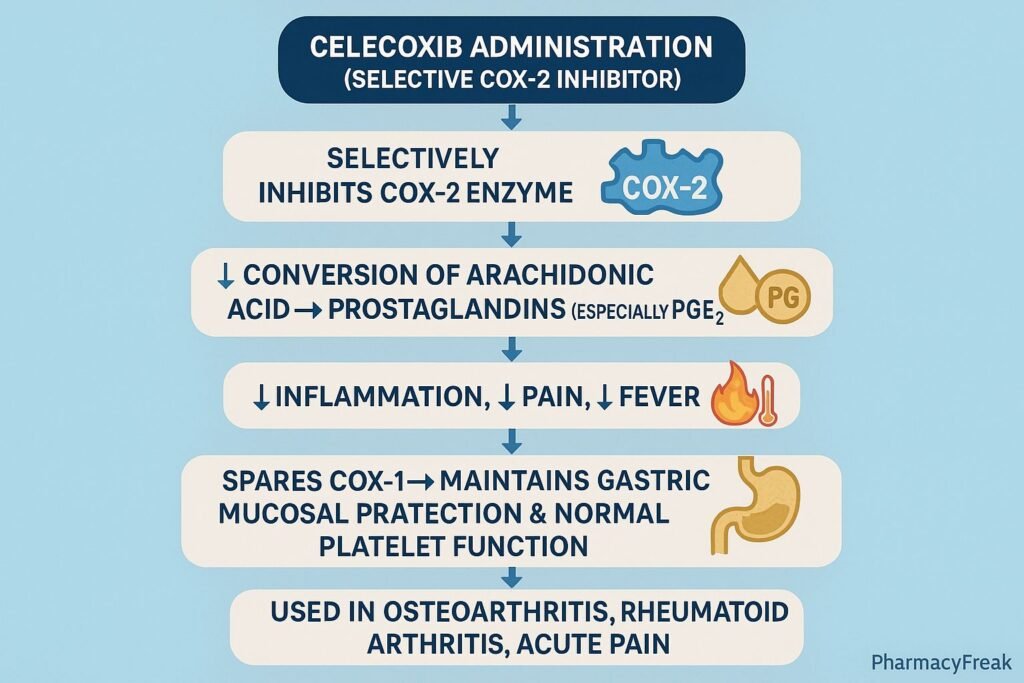
Celecoxib is a selective cyclooxygenase-2 (COX-2) inhibitor used widely for pain, inflammation, and osteoarthritis/rheumatoid arthritis management. Unlike nonselective NSAIDs, celecoxib spares COX-1, reducing the risks of gastric irritation and gastrointestinal bleeding while providing potent anti-inflammatory and analgesic effects.
The Mechanism of Action of Celecoxib centers on selective inhibition of COX-2, leading to decreased synthesis of inflammatory prostaglandins while preserving protective prostaglandins produced by COX-1.

Mechanism of Action (Step-wise)
1. Selective Inhibition of COX-2 – Primary Mechanism
COX-2 is an inducible enzyme expressed during:
- Inflammation
- Tissue injury
- Cytokine activation
Celecoxib selectively inhibits COX-2, thereby reducing the conversion of arachidonic acid to inflammatory prostaglandins (primarily PGE₂ and PGI₂).
Effects:
- Reduced inflammation
- Reduced pain perception
- Reduced swelling
- Improved joint function
2. Sparing of COX-1
COX-1 is constitutively active and produces:
- Gastric mucosal protective prostaglandins
- Platelet thromboxane (TXA₂)
- Renal blood flow regulators
Because celecoxib does not significantly inhibit COX-1, it causes:
- Less gastric ulceration
- Less gastrointestinal bleeding
- No effect on platelet aggregation
This gives celecoxib an improved GI safety profile.
3. Reduced Peripheral Sensitization
Lower PGE₂ levels lead to:
- Reduced nociceptor sensitivity
- Decreased inflammatory hyperalgesia
This results in potent analgesic action.
4. Modulation of Central Sensitization
Celecoxib can cross the blood–brain barrier and decrease central prostaglandin formation, reducing central sensitization to pain.
5. Cardiovascular Impact (Important Clinical Note)
Selective COX-2 inhibition decreases prostacyclin (PGI₂) without affecting thromboxane (TXA₂).
This creates a prothrombotic imbalance, contributing to:
- Increased risk of myocardial infarction
- Increased stroke risk
Thus, celecoxib must be used cautiously in patients with cardiovascular disease.
6. Summary of Mechanism
| Mechanism | Effect |
|---|---|
| COX-2 inhibition | ↓ Inflammatory prostaglandins |
| COX-1 sparing | ↓ Gastric toxicity |
| ↓ PGE₂ | ↓ Pain and inflammation |
| ↓ PGI₂ | ↑ Cardiovascular risk |
| No platelet effect | Safe for bleeding risk |
Pharmacokinetics
- Absorption: Well absorbed orally
- Bioavailability: 40%
- Metabolism: Hepatic via CYP2C9
- Half-life: 11 hours
- Protein binding: 97%
- Excretion: Renal and fecal
Clinical Uses
- Osteoarthritis
- Rheumatoid arthritis
- Ankylosing spondylitis
- Acute pain
- Primary dysmenorrhea
- Juvenile rheumatoid arthritis
- Familial adenomatous polyposis (reduces colorectal polyps)
Adverse Effects
Common
- Dyspepsia
- Abdominal pain
- Peripheral edema
- Headache
Serious
- Cardiovascular events (MI, stroke)
- Renal impairment
- Stevens–Johnson syndrome (rare)
- Hypertension
- Hepatotoxicity
Contraindications
- Sulfonamide allergy
- Severe cardiovascular disease
- Pregnancy (3rd trimester)
- GI bleeding history (use caution)
- Severe hepatic or renal impairment
Comparative Analysis
| Feature | Celecoxib | Ibuprofen | Aspirin |
|---|---|---|---|
| COX selectivity | COX-2 selective | Nonselective | COX-1 > COX-2 |
| GI safety | High | Moderate | Low |
| Platelet effect | None | Reversible inhibition | Irreversible inhibition |
| CV risk | Higher | Moderate | Lower in low dose |
| Use in arthritis | Excellent | Good | Limited by GI effects |
MCQs
1. Celecoxib acts primarily by inhibiting:
a) COX-1
b) COX-2
c) LOX pathway
d) Thromboxane synthase
Answer: b) COX-2
2. Celecoxib causes less gastric irritation because it:
a) Stimulates prostaglandins
b) Spares COX-1
c) Inhibits histamine release
d) Is not absorbed orally
Answer: b) Spares COX-1
3. Which adverse effect is increased with celecoxib use?
a) Bleeding
b) Cardiovascular risk
c) Hypotension
d) Hypokalemia
Answer: b) Cardiovascular risk
4. Platelet function is unaffected because celecoxib:
a) Inhibits serotonin
b) Does not inhibit COX-1
c) Inhibits thromboxane
d) Acts as an anticoagulant
Answer: b) Does not inhibit COX-1
5. Celecoxib is contraindicated in patients with:
a) Sulfonamide allergy
b) Mild hypertension
c) Seasonal allergy
d) Hypothyroidism
Answer: a) Sulfonamide allergy
FAQs
Q1. Why is celecoxib safer for the stomach?
Because it selectively inhibits COX-2 while sparing COX-1.
Q2. Does celecoxib increase heart attack risk?
Yes—due to reduced prostacyclin without affecting thromboxane.
Q3. Can celecoxib be given with aspirin?
Use caution; combination increases GI and cardiovascular risk.
Q4. Is celecoxib safe in sulfa allergy?
No—it is contraindicated.
Q5. Does celecoxib affect bleeding time?
No—it does not inhibit platelet COX-1.
References
Goodman & Gilman’s Pharmacological Basis of Therapeutics
https://accesspharmacy.mhmedical.com/book.aspx?bookid=2189
Katzung: Basic and Clinical Pharmacology
https://accessmedicine.mhmedical.com/book.aspx?bookid=2464
Tripathi: Essentials of Medical Pharmacology
https://jaypeebrothers.com/
Harrison’s Principles of Internal Medicine
https://accessmedicine.mhmedical.com/book.aspx?bookid=2129


