Table of Contents
Introduction
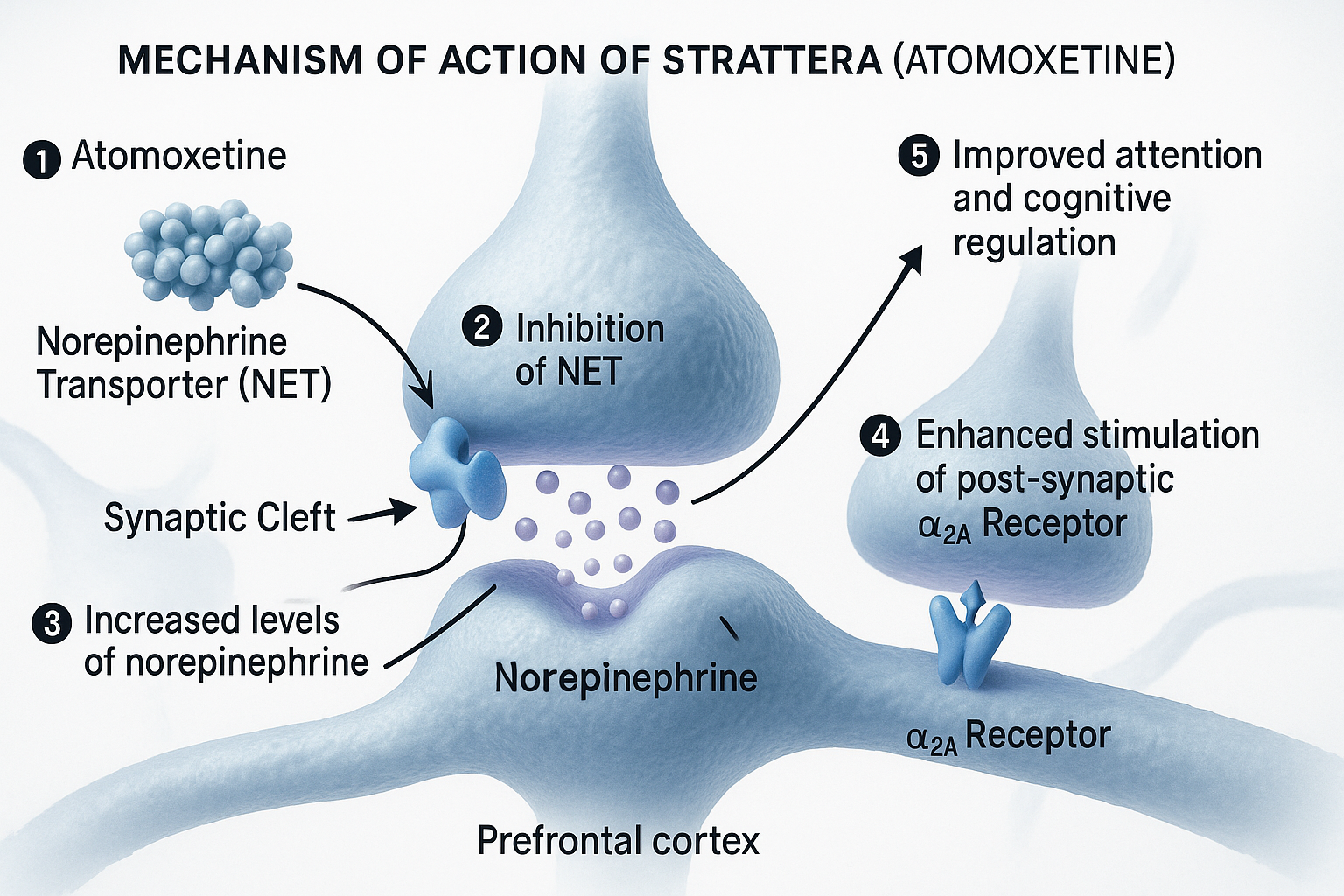
Strattera, the brand name for atomoxetine, is a non-stimulant medication used primarily in the treatment of attention-deficit hyperactivity disorder (ADHD). Unlike stimulant medications such as methylphenidate or amphetamines, atomoxetine works through selective modulation of norepinephrine.

Mechanism of Action (Stepwise Points)
- Selective Norepinephrine Reuptake Inhibition (NRI)
Atomoxetine selectively inhibits the norepinephrine transporter (NET), preventing the reuptake of norepinephrine into presynaptic neurons. - Increased Synaptic Norepinephrine
This results in elevated norepinephrine levels in the prefrontal cortex, an area associated with attention, behavior regulation, and executive function. - Modest Dopaminergic Modulation
Atomoxetine does not directly affect dopamine reuptake in the striatum but may indirectly enhance dopamine signaling in the prefrontal cortex due to NET inhibition. - Non-Stimulant Profile
Because it does not affect dopamine significantly in reward pathways, it has minimal abuse potential and lacks typical stimulant-associated side effects.


Pharmacokinetics
- Absorption: Well absorbed orally; peak plasma levels in 1–2 hours.
- Bioavailability: ~63%; affected by first-pass metabolism.
- Metabolism: Primarily metabolized by CYP2D6; extensive polymorphic variability.
- Half-life: ~5.2 hours in extensive metabolizers; up to 21 hours in poor metabolizers.
- Excretion: Primarily renal.
Clinical Uses
- Attention-deficit hyperactivity disorder (ADHD) in children, adolescents, and adults
- May be considered in patients with risk of substance abuse or stimulant intolerance
Adverse Effects
- Gastrointestinal disturbances (nausea, decreased appetite)
- Insomnia or somnolence
- Increased heart rate and blood pressure
- Mood swings or irritability
- Sexual dysfunction (especially in adults)
- Rare: Suicidal ideation (boxed warning)
Comparative Analysis
| Feature | Atomoxetine (Strattera) | Methylphenidate | Amphetamine |
|---|---|---|---|
| Drug Class | NRI | Dopamine/norepinephrine reuptake inhibitor | Dopamine/norepinephrine releaser |
| Abuse Potential | Low | Moderate | High |
| Onset of Action | Delayed (1–2 weeks) | Rapid (1 hour) | Rapid (30–60 min) |
| Duration | 24 hours | 4–12 hours | 6–12 hours |
| Primary Neurotransmitter | Norepinephrine | Dopamine & Norepinephrine | Dopamine & Norepinephrine |
Explanation: Atomoxetine is preferred in patients with a history of substance abuse or in those requiring 24-hour symptom control without stimulant-related side effects.
Multiple Choice Questions (MCQs)
- What is the primary mechanism of action of atomoxetine?
a) Dopamine release
b) Norepinephrine reuptake inhibition
c) Serotonin agonism
d) GABA-A modulation - Strattera is classified as a:
a) Stimulant
b) Non-stimulant
c) SSRI
d) MAOI - Which enzyme is primarily involved in atomoxetine metabolism?
a) CYP3A4
b) CYP2D6
c) CYP2C9
d) CYP1A2 - Strattera’s abuse potential is:
a) High
b) Low
c) Moderate
d) Comparable to methylphenidate - Common cardiovascular effect of atomoxetine:
a) Bradycardia
b) Increased heart rate
c) Hypotension
d) QT prolongation - Atomoxetine has the most significant effect in which brain region?
a) Striatum
b) Hippocampus
c) Prefrontal cortex
d) Cerebellum - One advantage of atomoxetine over stimulants is:
a) Stronger efficacy
b) No abuse potential
c) Immediate effect
d) Less expensive - Atomoxetine is especially preferred in patients with:
a) Depression
b) Obesity
c) Substance abuse risk
d) Schizophrenia - Atomoxetine onset of therapeutic action is typically:
a) Within 30 minutes
b) 1–2 weeks
c) 24 hours
d) 6–8 weeks - Atomoxetine may cause sexual dysfunction due to:
a) Dopaminergic excess
b) Norepinephrine modulation
c) Serotonin blockade
d) GABA activation
FAQs
Q1: Is atomoxetine a first-line treatment for ADHD?
A1: Yes, especially in patients who cannot tolerate or are at risk with stimulant use.
Q2: Can atomoxetine be used in adults?
A2: Yes, it is approved for ADHD in both children and adults.
Q3: Does it require titration?
A3: Yes, gradual dose escalation helps minimize side effects.
Q4: Is a drug holiday recommended?
A4: Not typically, since it requires continuous administration for efficacy.
References
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics, 12th Edition
- KD Tripathi, Essentials of Medical Pharmacology, 7th Edition
- Pharmacological Screening Methods & Toxicology by Avanapu Srinivasa Rao
- Biopharmaceutics & Pharmacokinetics by Thakur Publication


