Table of Contents
Introduction
SGLT2 inhibitors, also known as “gliflozins,” are a class of oral antidiabetic agents primarily used to manage type 2 diabetes mellitus. They also exhibit notable cardiovascular and renal protective effects, making them valuable in treating heart failure and chronic kidney disease, even in non-diabetic patients.
Step-by-Step Mechanism of Action
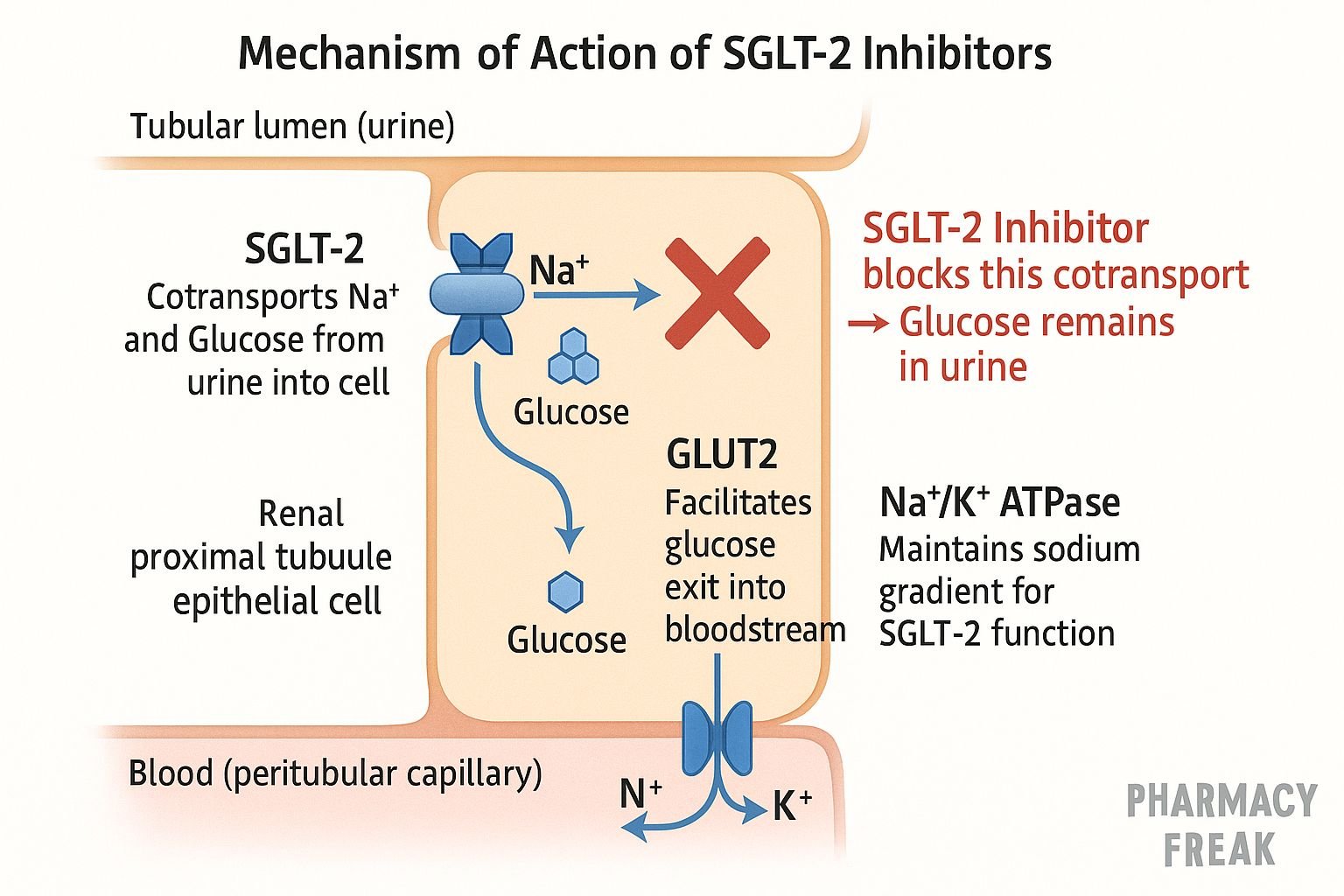
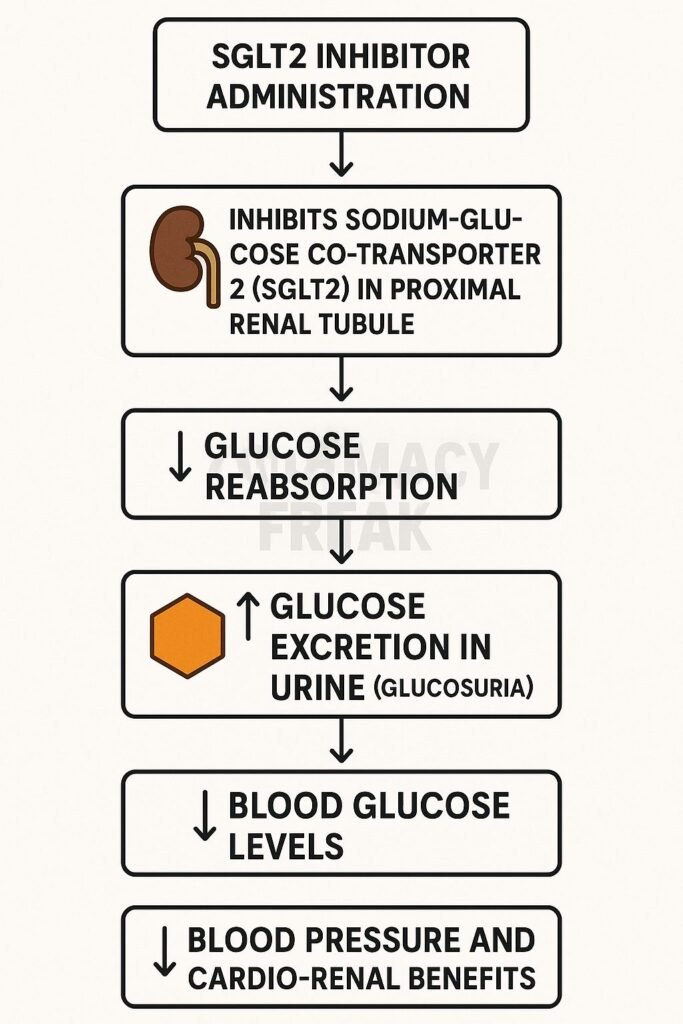
- Inhibition of SGLT2 in the Proximal Tubule
These drugs selectively block the sodium-glucose co-transporter 2 (SGLT2) in the early segment of the proximal convoluted tubule of the nephron. - Reduced Glucose Reabsorption
Normally, SGLT2 is responsible for reabsorbing approximately 90% of filtered glucose. Inhibition leads to increased urinary glucose excretion (glucosuria). - Osmotic Diuresis
The excretion of glucose in the urine pulls water with it, resulting in increased urine volume (osmotic diuresis) and modest natriuresis (sodium excretion). - Caloric Loss and Weight Reduction
Loss of glucose translates into a caloric deficit, contributing to modest weight loss in patients. - Improved Glycemic Control
Blood glucose levels decrease due to reduced glucose reabsorption, which helps lower HbA1c levels. - Enhanced Erythropoiesis and Hematocrit
Volume contraction and renal signaling promote erythropoietin release, leading to increased hematocrit and improved oxygen delivery. - Cardiovascular and Renal Protection
These drugs reduce intraglomerular pressure, albuminuria, and myocardial stress, improving outcomes in heart failure and slowing the progression of CKD.
Pharmacokinetic Parameters
| Parameter | Value |
|---|---|
| Absorption | High oral bioavailability (~70–90%) |
| Tmax | ~1 to 2 hours |
| Protein Binding | High (~86–99%) |
| Metabolism | Primarily glucuronidation (UGT enzymes) |
| Half-life | ~12 to 13 hours |
| Excretion | Renal and fecal routes |
Clinical Uses
- Type 2 diabetes mellitus (T2DM)
- Heart failure with reduced ejection fraction (HFrEF)
- Chronic kidney disease (CKD), including non-diabetics
Adverse Effects
- Genital mycotic infections
- Urinary tract infections
- Volume depletion, hypotension
- Euglycemic diabetic ketoacidosis (rare)
- Increased LDL cholesterol
- Rare risk of Fournier’s gangrene (especially with canagliflozin)
Comparative Analysis
| Drug | SGLT2 Selectivity | Key Features |
|---|---|---|
| Empagliflozin | High | Strong CV protection, once-daily dosing |
| Dapagliflozin | High | Broadest approved indications (DM, HF, CKD) |
| Canagliflozin | Moderate | Slight SGLT1 activity, amputation risk noted |
MCQs
- SGLT2 inhibitors act on which part of the nephron?
a) Distal tubule b) Loop of Henle c) Collecting duct d) Proximal tubule
Answer: d) Proximal tubule - Primary action of SGLT2 inhibitors is:
a) Increasing insulin secretion b) Reducing glucose reabsorption c) Enhancing glucose uptake d) Inhibiting hepatic gluconeogenesis
Answer: b) Reducing glucose reabsorption - Which of the following is a common side effect?
a) Hypernatremia b) Genital infections c) Bradycardia d) Hypercalcemia
Answer: b) Genital infections - Glucosuria leads to:
a) Fluid retention b) Hyponatremia c) Osmotic diuresis d) Metabolic alkalosis
Answer: c) Osmotic diuresis - Cardiovascular benefit of SGLT2 inhibitors includes:
a) Increased preload b) Reduced heart failure hospitalization c) Increased LDL d) Worsened ejection fraction
Answer: b) Reduced heart failure hospitalization - Which drug has additional SGLT1 inhibition?
a) Empagliflozin b) Dapagliflozin c) Canagliflozin d) Ertugliflozin
Answer: c) Canagliflozin - Metabolism primarily occurs via:
a) CYP3A4 b) Glucuronidation c) Sulfation d) Oxidation
Answer: b) Glucuronidation - Which serious condition can occur despite normal blood glucose levels?
a) Hyperosmolar coma b) Euglycemic ketoacidosis c) Lactic acidosis d) Hemolysis
Answer: b) Euglycemic ketoacidosis - Albuminuria reduction is due to:
a) Increased GFR b) Reduced intraglomerular pressure c) Enhanced filtration d) Sodium retention
Answer: b) Reduced intraglomerular pressure - Which is a contraindication for SGLT2 inhibitors?
a) Type 2 diabetes b) CKD stage 2 c) Type 1 diabetes d) Hypertension
Answer: c) Type 1 diabetes
FAQs
1. Can SGLT2 inhibitors be used in type 1 diabetes?
No, they are contraindicated due to the risk of euglycemic ketoacidosis.
2. Do they help in heart failure patients without diabetes?
Yes, especially in HFrEF and CKD, even in non-diabetics.
3. Is there a risk of hypoglycemia?
Minimal when used alone, but risk increases with insulin or sulfonylureas.
4. Do they require renal function monitoring?
Yes, efficacy decreases with low eGFR and dose adjustment may be needed.
5. Do they reduce weight?
Yes, through caloric loss from urinary glucose excretion.
References
- PubMed: SGLT2 Inhibitor Review – PMC8720766
- PubMed: Cardiovascular & Renal Mechanisms – PMID: 39017631
- DrugBank: SGLT2 Inhibitors Overview
- StatPearls: SGLT2 Inhibitors
- MDPI: Pleiotropic Effects of SGLT2 Inhibitors

I am pursuing MBA in pharmaceutical management from NIPER Hyderabad with a strong academic record and proven success in national-level pharmacy entrance exams. I secured AIR 61 in NIPER 2024 (MS/M.Pharm) and AIR 27 in NIPER MBA, along with AIR 147 in GPAT 2024 and AIR 907 in GPAT 2023. I also achieved AIR 6 in AIIMS CRE-2025 for Drug Store Keeper and was selected as a Pharmacist (AIR 61) for ESIC. Additionally, I was the Runner-Up in Round 2 of the EY Case Study Competition.
At PharmacyFreak.com, I aim to guide future pharmacists through expert content, exam strategies, and insightful resources based on real experience and academic excellence.
Mail- harsh@pharmacyfreak.com