Semaglutide (Ozempic for diabetes; Wegovy for obesity) is a GLP‑1 receptor agonist used for type 2 diabetes mellitus management and chronic weight loss. It mimics the incretin hormone glucagon‑like peptide‑1 (GLP‑1), leading to improved glycemic control, reduced appetite, delayed gastric emptying, and favorable effects on cardiovascular risk.
Step-by-Step Mechanism of Action
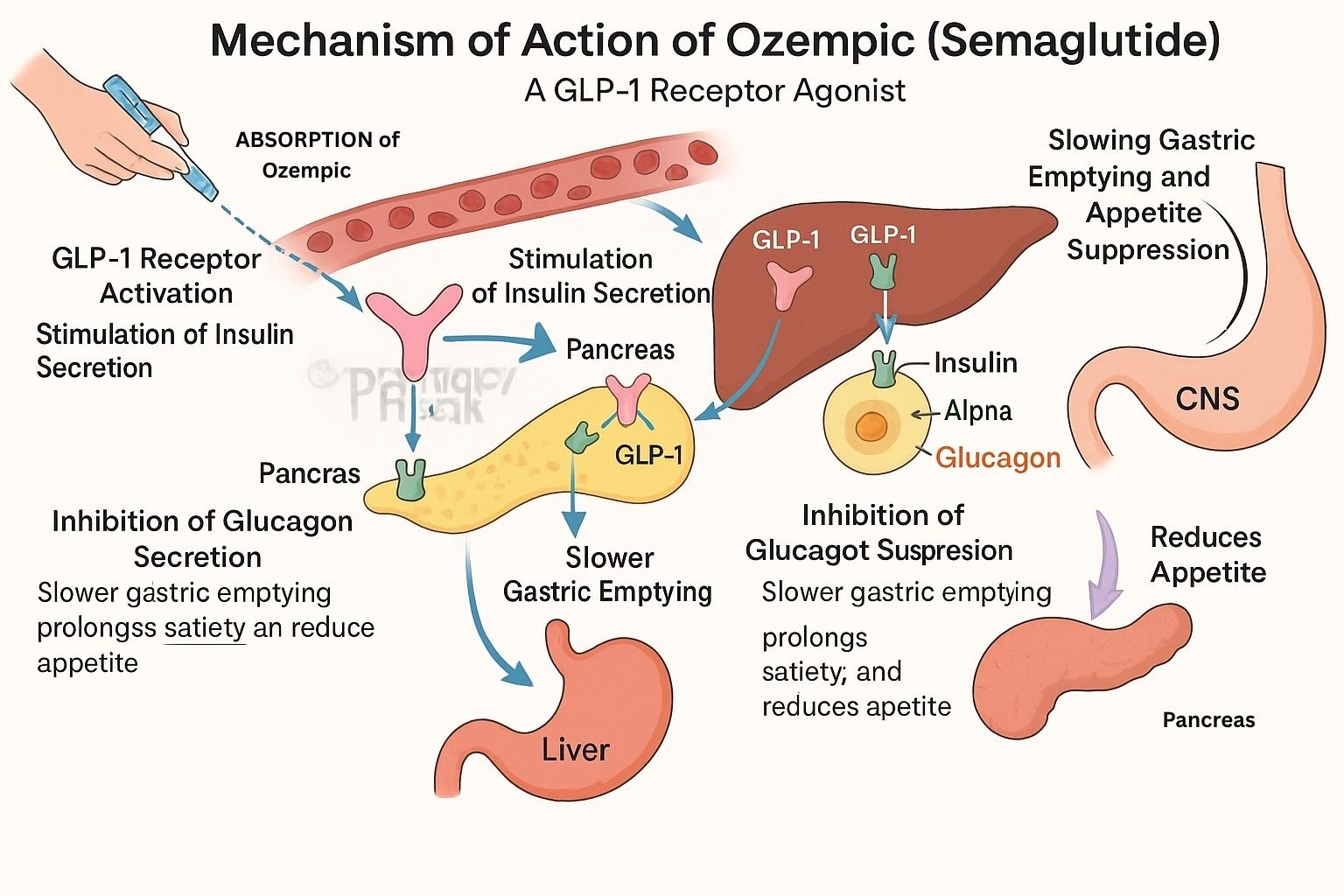
GLP‑1 receptor activation Semaglutide binds to GLP‑1 receptors on pancreatic β‑cells and brain centers, mimicking endogenous GLP‑1.
Glucose-dependent insulin secretion Receptor activation increases cAMP in β‑cells, enhancing insulin release when blood glucose is elevated.
Glucagon suppression It inhibits glucagon secretion from α‑cells, reducing hepatic glucose production.
Delayed gastric emptying Acting on GLP‑1 receptors in the gut and brain delays gastric emptying, prolonging satiety and reducing postprandial glucose spikes.
Appetite reduction and weight loss Central effects on the hypothalamus and brain stem decrease appetite and caloric intake, promoting weight loss.
Potential cardiovascular benefits GLP‑1 receptor effects on endothelial and cardiac tissues may improve vascular health and reduce risk of major cardiovascular events.
Mechanism of Action of ozempic flowchart
Pharmacokinetic Parameters
Parameter
Value
Route
Subcutaneous injection, weekly (Ozempic) or weekly/higher doses for Wegovy
Bioavailability
~80–90%
Time to Peak (Tmax)
~1–3 days
Half-life
~7 days
Metabolism
Proteolytic degradation; no CYP involvement
Excretion
Urine (~3%), feces (~5%), remainder via metabolism
Clinical Uses
Primary treatment of type 2 diabetes mellitus to reduce HbA₁c
Chronic weight management in obesity or overweight individuals with risk factors
Reduces risk of major adverse cardiovascular events in high-risk diabetic patients
Adverse Effects
Common: nausea, diarrhea, constipation, vomiting
Less common: injection-site reactions, headache, dizziness
Rare risk: pancreatitis; monitor for gallbladder disease
Caution: use in patients with a history of medullary thyroid carcinoma or MEN2
Comparative Analysis
Agent
Receptor Target
HbA₁c Reduction
Weight Loss
Administration Frequency
Semaglutide
GLP‑1 agonist
1.5–2.3%
10–17%
Weekly injection
Liraglutide
GLP‑1 agonist
~1.0–1.5%
~7–10%
Daily injection
Exenatide
GLP‑1 agonist
~0.8–1.1%
~3–5%
Twice daily or weekly
MCQs (15)
Semaglutide primarily acts on which receptor? a) GIP receptor b) GLP‑1 receptor c) Insulin receptor d) DPP‑4 receptor Answer: b) GLP‑1 receptor
It enhances insulin secretion in a _____ manner. a) Glucose-dependent b) Constant c) Glucose-independent d) Time-dependent Answer: a) Glucose-dependent
It suppresses which hormone? a) Somatostatin b) Glucagon c) Ghrelin d) Cortisol Answer: b) Glucagon
Typical onset of gastric emptying delay is: a) Within minutes b) Within hours c) After weeks d) No effect Answer: b) Within hours
Semaglutide injection frequency is: a) Daily b) Weekly c) Monthly d) As-needed Answer: b) Weekly
A rare but serious adverse effect to monitor is: a) Hypoglycemia b) Pancreatitis c) Hyperthyroidism d) Nephrolithiasis Answer: b) Pancreatitis
It is contraindicated in patients with: a) Type 1 diabetes b) Medullary thyroid carcinoma c) Obesity d) Hypertension Answer: b) Medullary thyroid carcinoma
Compared to exenatide, semaglutide yields: a) Less weight loss b) More weight loss c) Higher injection frequency d) Less HbA₁c reduction Answer: b) More weight loss
Half-life of semaglutide is approximately: a) 24 hours b) 3 days c) 7 days d) 15 days Answer: c) 7 days
Excretion involves: a) High renal elimination b) Only feces c) Metabolism and minimal excretion d) Biliary excretion Answer: c) Metabolism and minimal excretion
An added cardiovascular benefit was shown in: a) SUSTAIN trials b) DPP‑4 studies c) RAAS inhibitor trials d) REM sleep studies Answer: a) SUSTAIN trials
Weight loss percentage ranges from: a) 1–5% b) 5–10% c) 10–17% d) 20–25% Answer: c) 10–17%
A significant GI side effect is: a) Increased appetite b) Nausea c) Insomnia d) Hypertension Answer: b) Nausea
Semaglutide metabolism involves: a) CYP3A4 b) Proteolysis c) Renal enzymes only d) Conjugation Answer: b) Proteolysis
An advantage over liraglutide is: a) Lower efficacy b) Higher weight loss c) Daily dosing d) Less frequent injection Answer: d) Less frequent injection
FAQs
Does semaglutide cause weight loss in non-diabetic patients? Yes—it’s approved for chronic weight management under Wegovy, showing 10–17% loss.
How soon does glycemic control improve? HbA₁c reduction is often seen within 4–8 weeks.
Can semaglutide be combined with insulin? Yes—with adjustment; monitor for hypoglycemia.
Is cardiovascular benefit proven? Yes—major trials showed reductions in cardiovascular events in diabetic patients.
Does semaglutide need dose titration? Yes—gradual dose escalation helps improve tolerance, especially GI.
Harsh Singh Rajput is a pharmacist currently working at ESIC and holds an MBA in Pharmaceutical Management from NIPER Hyderabad. He has a strong academic record with top ranks in national-level pharmacy exams, including AIR 61 in NIPER 2024 (MS/M.Pharm), AIR 27 in NIPER MBA, AIR 147 in GPAT 2024, AIR 907 in GPAT 2023, and AIR 6 in AIIMS CRE-2025 for Drug Store Keeper. At PharmacyFreak.com, he contributes expert content, exam strategies, and practical guidance for future pharmacists.
Mail- harsh@pharmacyfreak.com