Table of Contents
Introduction
Omeprazole is a commonly prescribed drug used to reduce gastric acid secretion. It belongs to the class of proton pump inhibitors (PPIs) and is widely used in the treatment of acid-related disorders. Due to its superior efficacy and tolerability, it has largely replaced H2 blockers in clinical practice.
Omeprazole is primarily indicated in:
- Peptic ulcer disease
- Gastroesophageal reflux disease (GERD)
- Zollinger-Ellison syndrome
- Helicobacter pylori eradication (as part of combination therapy)
Understanding its mechanism of action is crucial for students of medical and pharmacy sciences and for success in competitive exams like GPAT, NEET-PG, NIPER, and NCLEX.
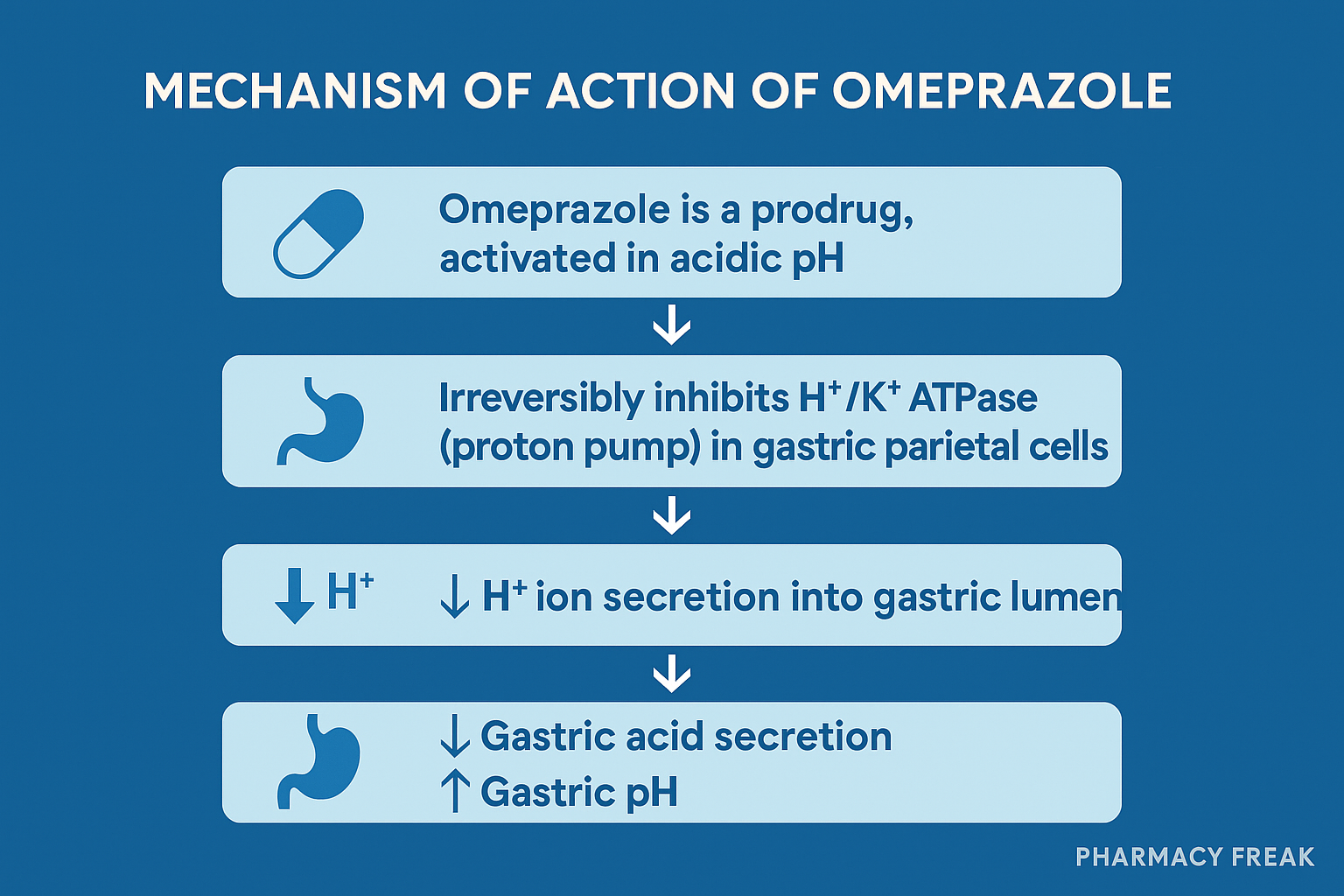
Stepwise Mechanism of Action of Omeprazole
- Prodrug Activation in Acidic Environment
Omeprazole is a prodrug that is acid-labile and requires activation in the acidic environment of the parietal cell canaliculi. It is administered in an enteric-coated formulation to prevent degradation in the stomach. - Conversion to Active Sulfenamide
Once inside the parietal cells, it is converted to its active form, a sulfenamide derivative, in the acidic secretory canaliculus. - Covalent Binding to H+/K+ ATPase
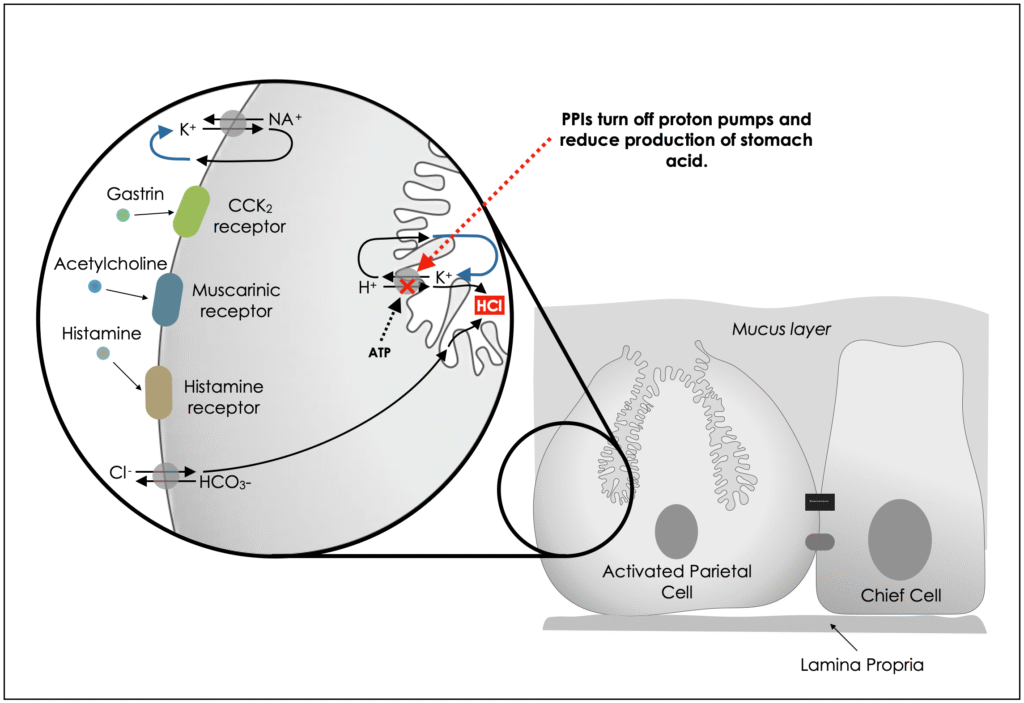
The activated omeprazole binds irreversibly to the sulfhydryl group of H+/K+ ATPase (the proton pump) located on the luminal surface of parietal cells. This enzyme is the final step in the acid secretion pathway. - Inhibition of Gastric Acid Secretion
By blocking the proton pump, omeprazole inhibits both basal and stimulated gastric acid secretion, regardless of the stimulus (histamine, gastrin, or acetylcholine). - Irreversibility and Long Duration
Since binding is irreversible, acid secretion resumes only after new proton pumps are synthesized, leading to a long duration of action despite a short plasma half-life.
Pharmacokinetic Parameters of Omeprazole
| Parameter | Value |
|---|---|
| Bioavailability | ~35–40% (increases with repeated dosing) |
| Onset of Action | 1 hour (max effect in 2 hours) |
| Half-life | 0.5 to 1 hour (but long effect due to irreversible action) |
| Protein Binding | ~95% |
| Metabolism | Hepatic via CYP2C19 and CYP3A4 |
| Excretion | Renal and fecal (as inactive metabolites) |
Clinical Uses of Omeprazole
- Gastroesophageal reflux disease (GERD)
- Peptic ulcer disease (gastric and duodenal ulcers)
- Erosive esophagitis
- Zollinger-Ellison syndrome (gastrinoma)
- Helicobacter pylori eradication (as part of triple therapy)
- NSAID-induced gastric injury prevention
Adverse Effects of Omeprazole
- Headache, nausea, diarrhea
- Abdominal pain, constipation
- Long-term use risks:
- Vitamin B12 deficiency
- Hypomagnesemia
- Increased risk of bone fractures
- Increased risk of enteric infections (e.g., C. difficile)
- Possible increased risk of gastric cancer with prolonged use
Comparative Analysis: Omeprazole vs Ranitidine
| Feature | Omeprazole (PPI) | Ranitidine (H2 blocker) |
|---|---|---|
| Site of Action | H+/K+ ATPase (proton pump) | H2 receptor on parietal cells |
| Acid Suppression | Profound and long-lasting | Moderate and short-lasting |
| Onset of Action | Slow (1–2 hours) | Rapid (within 30 minutes) |
| Duration of Action | >24 hours | 6–10 hours |
| Inhibition Type | Irreversible | Reversible |
| Effect on Basal Acid | Strong | Moderate |
| Role in H. pylori Therapy | Yes | No |
Practice MCQs
Q1. Omeprazole inhibits which of the following enzymes?
A. HMG-CoA reductase
B. Na+/K+ ATPase
C. H+/K+ ATPase
D. Carbonic anhydrase
Answer: C
Q2. What is the mechanism of omeprazole action?
A. Reversible inhibition of H2 receptor
B. Irreversible inhibition of proton pump
C. Inhibition of dopamine receptors
D. Activation of bicarbonate secretion
Answer: B
Q3. Omeprazole is activated in which part of the body?
A. Liver
B. Stomach lumen
C. Parietal cell canaliculi
D. Intestinal mucosa
Answer: C
Q4. Which of the following statements about omeprazole is false?
A. It has a long half-life
B. It is a prodrug
C. It binds irreversibly to H+/K+ ATPase
D. It is used in GERD
Answer: A
Q5. Omeprazole should be administered:
A. With a high-fat meal
B. With milk
C. On an empty stomach
D. At bedtime
Answer: C
Q6. A long-term risk of omeprazole therapy includes:
A. Hypokalemia
B. Hypomagnesemia
C. Hypernatremia
D. Hypercalcemia
Answer: B
Q7. Omeprazole is mainly metabolized by:
A. CYP2D6
B. CYP2E1
C. CYP2C19 and CYP3A4
D. CYP1A2
Answer: C
Q8. The acid-labile nature of omeprazole is addressed by:
A. IV formulation
B. Prolonged-release coating
C. Enteric coating
D. pH buffering
Answer: C
Q9. Omeprazole can increase the risk of which infection?
A. Influenza
B. Helicobacter pylori
C. Clostridium difficile
D. Shigella
Answer: C
Q10. Which of the following is a unique feature of omeprazole compared to H2 blockers?
A. Requires frequent dosing
B. Irreversible inhibition of proton pumps
C. Acts within 15 minutes
D. Causes sedation
Answer: B
FAQs
Q1: Is omeprazole safe for long-term use?
Short-term use is safe. Long-term use may lead to nutrient deficiencies and increased risk of infections and fractures.
Q2: Can omeprazole be used in pregnancy?
It is generally considered safe (Category C), but should be used under medical supervision.
Q3: How soon does omeprazole start working?
It starts reducing acid within 1 hour, but maximum effect is seen in 2–3 days.
Q4: What is the best time to take omeprazole?
It should be taken once daily on an empty stomach, ideally 30–60 minutes before breakfast.
References
- KD Tripathi – Essentials of Medical Pharmacology
- Goodman & Gilman – The Pharmacological Basis of Therapeutics
- Sparsh Gupta – Review of Pharmacology

