Table of Contents
Introduction
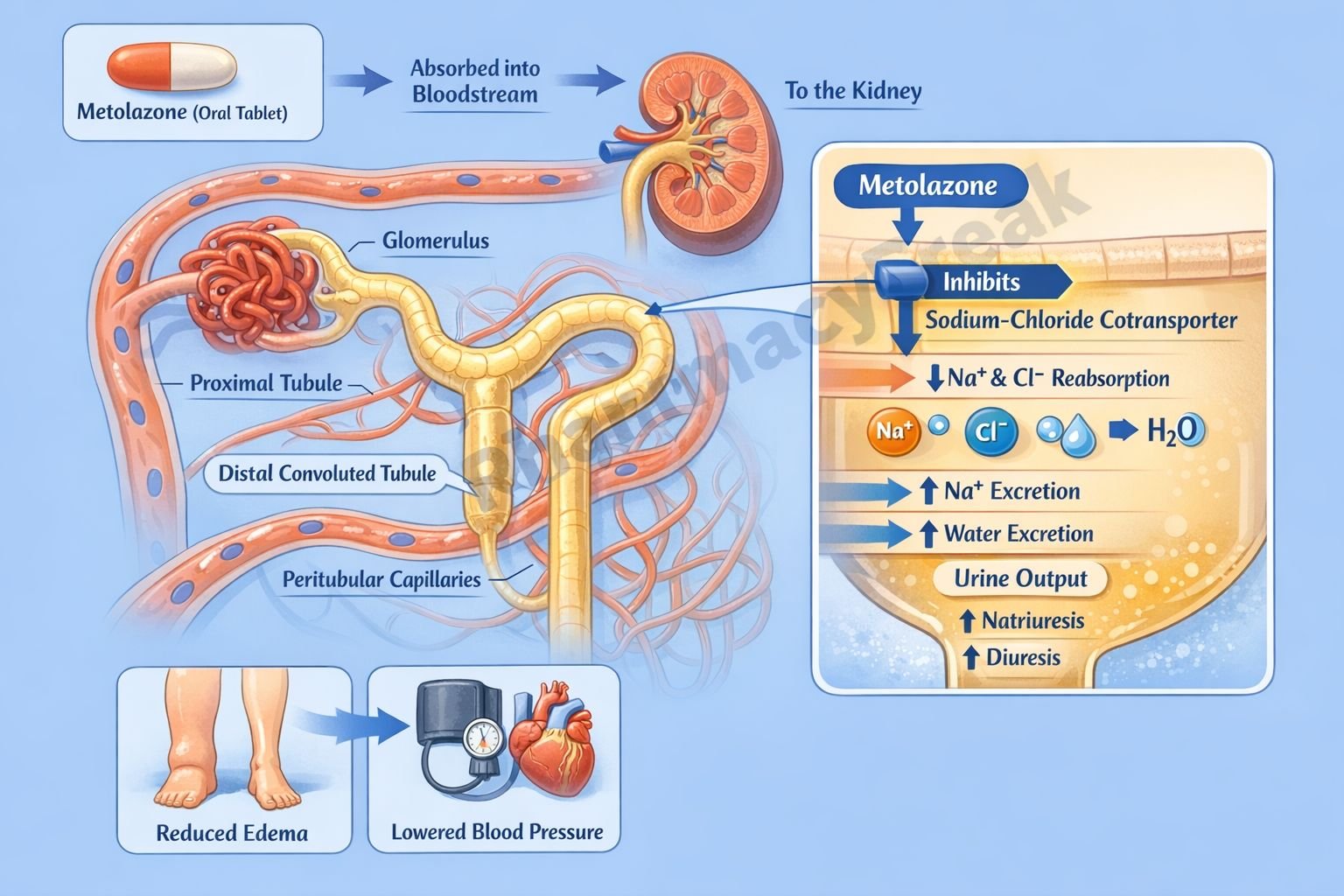
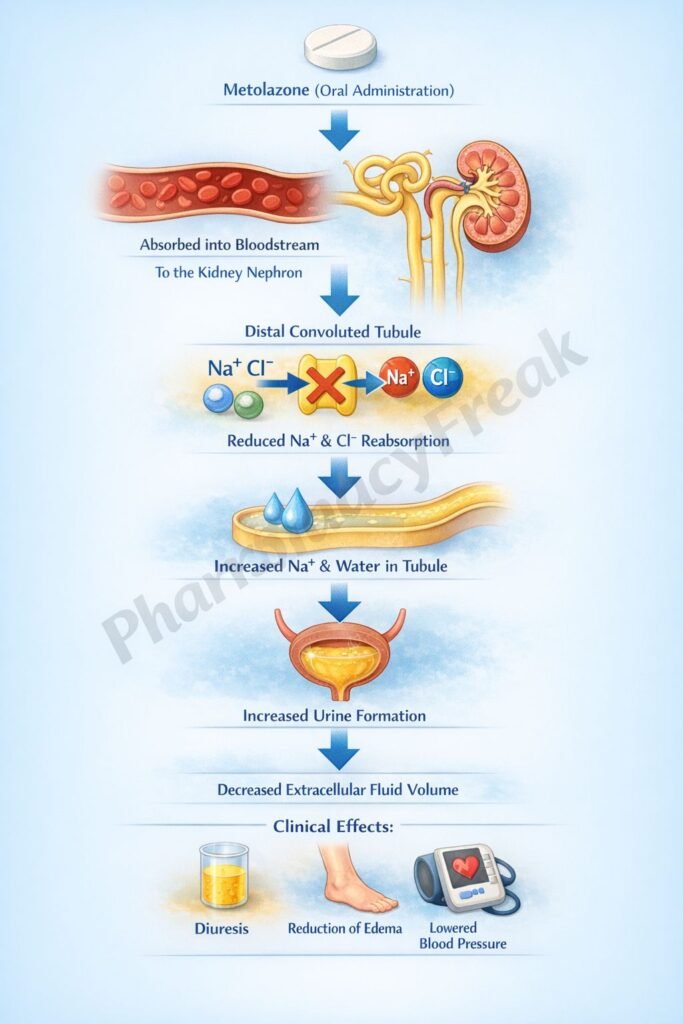
Metolazone is a thiazide-like diuretic commonly used in the management of hypertension and edema, particularly in patients with heart failure or chronic kidney disease. It is especially useful when combined with loop diuretics in resistant edema. Metolazone acts primarily on the distal convoluted tubule of the nephron to promote sodium and water excretion.
Mechanism of Action (Step-wise)
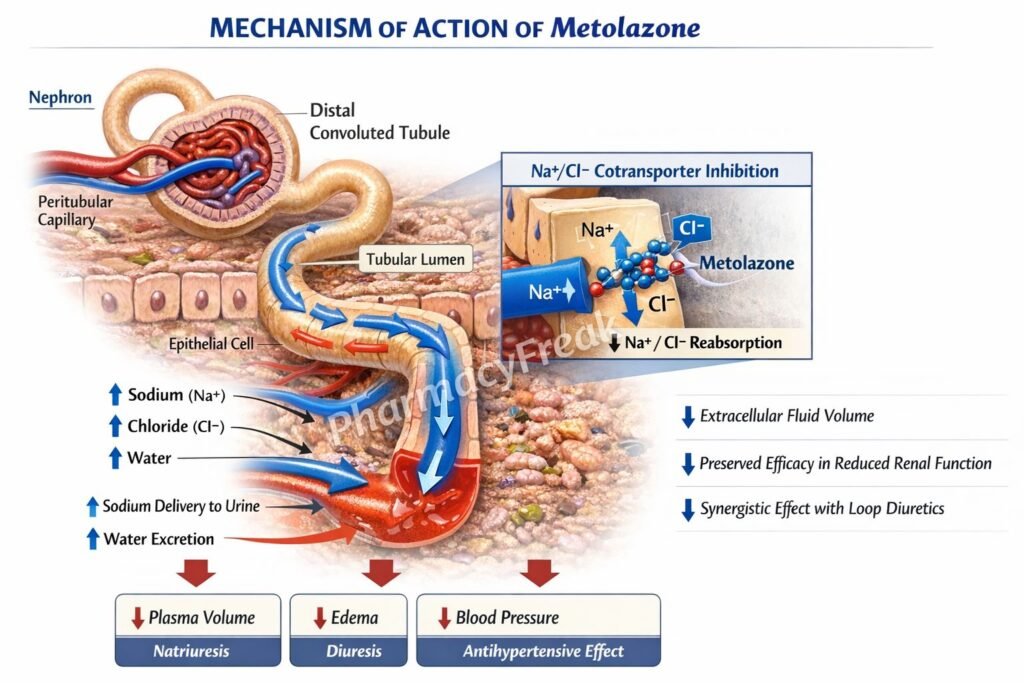
- Metolazone acts on the distal convoluted tubule (DCT) of the nephron.
- It inhibits the sodium-chloride (Na⁺/Cl⁻) symporter located on the luminal membrane.
- This reduces reabsorption of sodium and chloride from the tubular fluid.
- Increased sodium concentration in the tubular lumen leads to increased water excretion.
- This results in diuresis and reduction in extracellular fluid volume.
- Increased sodium delivery to the collecting duct enhances potassium and hydrogen ion excretion.
- This may lead to hypokalemia and metabolic alkalosis.
- Long-term use reduces peripheral vascular resistance, contributing to antihypertensive effects.
- It remains effective even at lower glomerular filtration rates compared to traditional thiazides.
A key exam point is that metolazone inhibits the Na⁺/Cl⁻ symporter in the distal convoluted tubule.
Pharmacokinetics
Metolazone is administered orally and is well absorbed. It has a relatively long duration of action compared to many other thiazide diuretics. It is metabolized minimally and is excreted mainly via the kidneys. Unlike typical thiazides, it retains effectiveness in patients with reduced renal function. Its prolonged action allows once-daily dosing in many cases.
Clinical Uses
Metolazone is used in the treatment of hypertension and edema associated with congestive heart failure, renal disease, and liver cirrhosis. It is particularly valuable in patients with diuretic resistance when used in combination with loop diuretics. This combination produces a synergistic effect by blocking sodium reabsorption at different nephron sites.
Adverse Effects
Common adverse effects include hypokalemia, hyponatremia, dehydration, and hypotension. Hyperuricemia may occur, increasing the risk of gout. Hyperglycemia and dyslipidemia may also be seen. Electrolyte imbalance is a major concern and requires monitoring during therapy.
Comparative Analysis
| Feature | Metolazone | Hydrochlorothiazide | Furosemide |
|---|---|---|---|
| Class | Thiazide-like diuretic | Thiazide diuretic | Loop diuretic |
| Site of action | Distal convoluted tubule | Distal convoluted tubule | Thick ascending limb |
| Mechanism | Na⁺/Cl⁻ inhibition | Na⁺/Cl⁻ inhibition | NKCC2 inhibition |
| Effect in renal failure | Effective | Less effective | Effective |
| Potency | Moderate | Moderate | High |
| Use | Resistant edema, hypertension | Hypertension | Severe edema |
Metolazone differs from hydrochlorothiazide by being effective even in patients with reduced renal function. Compared to furosemide, it is less potent but works synergistically when combined with loop diuretics, making it valuable in resistant edema.
MCQs
- Metolazone belongs to which class?
a) Loop diuretics
b) Thiazide-like diuretics
c) Potassium-sparing diuretics
d) Osmotic diuretics
Answer: b) Thiazide-like diuretics
- Metolazone acts on which part of the nephron?
a) Proximal tubule
b) Loop of Henle
c) Distal convoluted tubule
d) Collecting duct
Answer: c) Distal convoluted tubule
- Metolazone inhibits which transporter?
a) Na⁺/K⁺ ATPase
b) Na⁺/Cl⁻ symporter
c) NKCC2
d) ENaC
Answer: b) Na⁺/Cl⁻ symporter
- Metolazone increases excretion of:
a) Sodium and water
b) Glucose
c) Protein
d) Calcium only
Answer: a) Sodium and water
- Increased sodium delivery to collecting duct leads to:
a) Hypokalemia
b) Hyperkalemia
c) Hypernatremia
d) Hypocalcemia
Answer: a) Hypokalemia
- Metolazone is particularly useful in:
a) Asthma
b) Resistant edema
c) Diabetes
d) Thyroid disease
Answer: b) Resistant edema
- Compared to thiazides, metolazone is effective in:
a) Normal kidney function only
b) Renal failure
c) Liver failure only
d) Brain disorders
Answer: b) Renal failure
- A common adverse effect is:
a) Hyperkalemia
b) Hypokalemia
c) Hypercalcemia
d) Hypoglycemia
Answer: b) Hypokalemia
- Metolazone is used with loop diuretics for:
a) Antagonism
b) Synergistic effect
c) No effect
d) Reduced action
Answer: b) Synergistic effect
- Metolazone reduces blood pressure by:
a) Increasing cardiac output
b) Reducing fluid volume
c) Increasing sodium retention
d) Increasing heart rate
Answer: b) Reducing fluid volume
- Hyperuricemia may lead to:
a) Diabetes
b) Gout
c) Hypertension
d) Anemia
Answer: b) Gout
- Metolazone is administered:
a) Intravenously
b) Orally
c) Intramuscularly
d) Inhaled
Answer: b) Orally
FAQs
What is the mechanism of action of metolazone?
It inhibits the Na⁺/Cl⁻ symporter in the distal convoluted tubule, increasing sodium and water excretion.
Why is metolazone useful in resistant edema?
Because it works synergistically with loop diuretics and remains effective in renal impairment.
What electrolyte imbalance is common with metolazone?
Hypokalemia.
Can metolazone be used in renal failure?
Yes, it remains effective even with reduced kidney function.
What is a common adverse effect related to uric acid?
Hyperuricemia leading to gout.
How does metolazone lower blood pressure?
By reducing extracellular fluid volume and vascular resistance.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics – Diuretics
https://accessmedicine.mhmedical.com/book.aspx?bookid=3191
Katzung: Basic and Clinical Pharmacology – Diuretics
https://accessmedicine.mhmedical.com/content.aspx?bookid=3382
Tripathi: Essentials of Medical Pharmacology – Diuretics
https://www.jaypeedigital.com
Harrison’s Principles of Internal Medicine – Hypertension and Edema
https://accessmedicine.mhmedical.com

