Table of Contents
Introduction
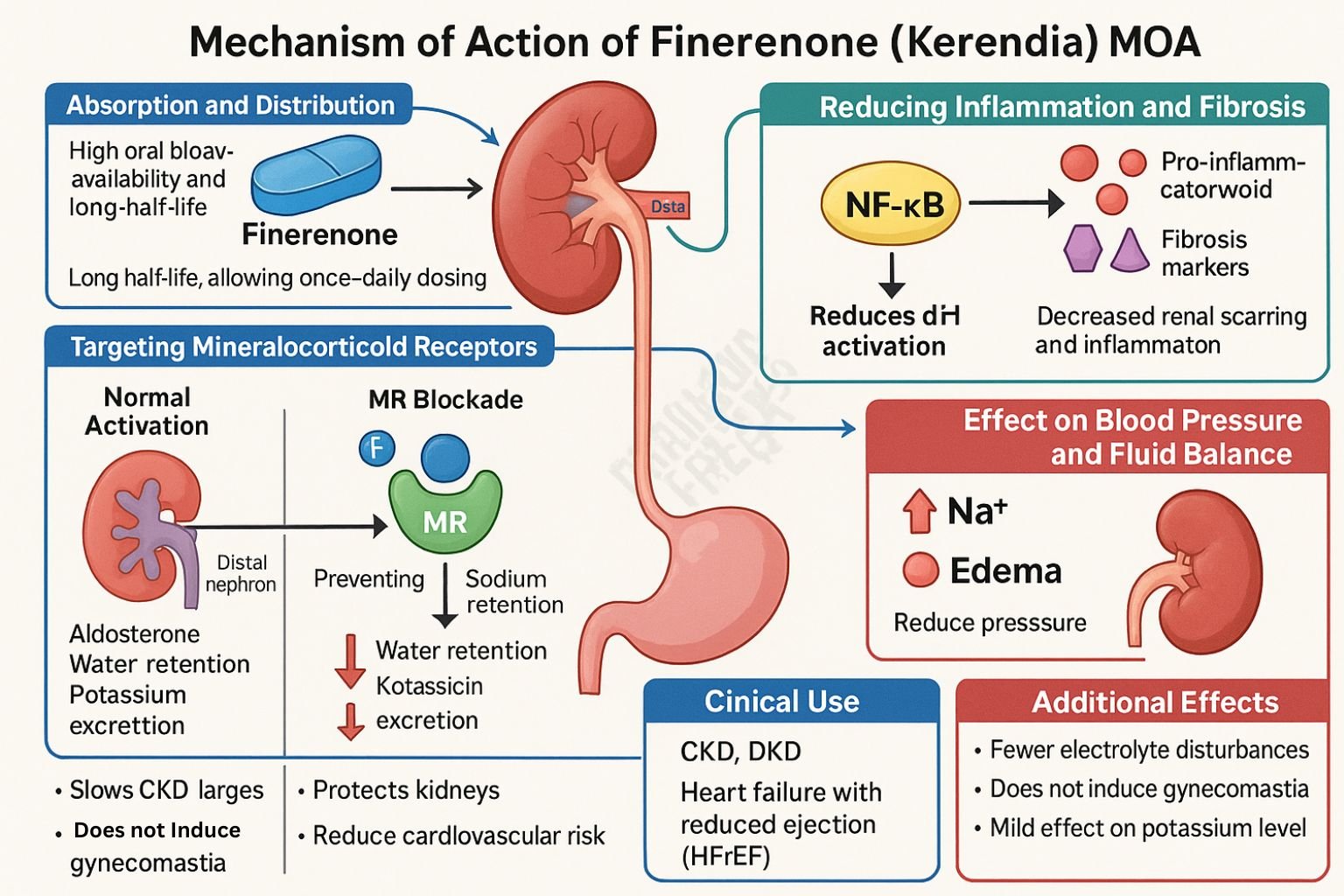
Finerenone is a nonsteroidal, selective mineralocorticoid receptor antagonist (MRA) approved for reducing the risk of cardiovascular and renal events in adults with chronic kidney disease (CKD) associated with type 2 diabetes mellitus (T2DM). Unlike steroidal MRAs such as spironolactone, finerenone offers greater mineralocorticoid receptor selectivity, minimizing off-target hormonal effects.
Step-by-Step Mechanism of Action
- High-Affinity MR Antagonism
Finerenone binds to the mineralocorticoid receptor (MR) with high affinity, blocking aldosterone-mediated activation of the receptor. - Inverse Agonism and Coactivator Blockade
Finerenone induces a unique MR conformation that inhibits recruitment of transcriptional coactivators, preventing activation of downstream aldosterone-responsive genes. - Anti-inflammatory and Antifibrotic Effects
By preventing MR-driven gene transcription, finerenone suppresses pro-inflammatory and pro-fibrotic signaling in renal and cardiac tissues. - Cardiorenal Protection
These actions stabilize kidney function by reducing albuminuria and also inhibit adverse cardiac remodeling, offering dual organ protection.

Pharmacokinetic Parameters
| Parameter | Value |
|---|---|
| Route | Oral |
| Time to peak (Tmax) | ~1.5 hours |
| Bioavailability | High |
| Protein Binding | ~92% |
| Half-life | ~2–3 hours |
| Metabolism | CYP3A4 (primary), CYP2C8 (minor) |
| Excretion | Renal and fecal |
Clinical Uses
- Management of CKD in patients with T2DM to slow progression to end-stage kidney disease
- Reduction of cardiovascular mortality and hospitalization in high-risk patients with CKD and diabetes
- Potential use in heart failure with preserved ejection fraction (HFpEF) under clinical evaluation
Adverse Effects
- Hyperkalemia (dose-dependent; monitor serum potassium)
- Hypotension
- Hyponatremia (less common)
- No anti-androgenic or gynecomastia effects due to high MR selectivity
Comparative Analysis
| Drug | MR Selectivity | Half-Life | Cardiorenal Benefits | Hyperkalemia Risk |
|---|---|---|---|---|
| Spironolactone | Low | >20 hours | Yes | High |
| Eplerenone | Moderate | 4–6 hours | Yes | Moderate |
| Finerenone | High | 2–3 hours | Yes | Lower |
MCQs
1. Finerenone is best classified as:
a) Steroidal MRA
b) Nonsteroidal MRA
c) ACE inhibitor
d) ARB
Answer: b) Nonsteroidal MRA
2. The primary receptor targeted by finerenone is:
a) Glucocorticoid receptor
b) Aldosterone synthase
c) Mineralocorticoid receptor
d) Androgen receptor
Answer: c) Mineralocorticoid receptor
3. Finerenone’s action prevents:
a) MR gene activation
b) Calcium absorption
c) Sodium excretion
d) RAAS inactivation
Answer: a) MR gene activation
4. Its anti-inflammatory effect is due to:
a) Sodium channel inhibition
b) COX inhibition
c) Gene transcription suppression
d) GABA modulation
Answer: c) Gene transcription suppression
5. What is the main organ system benefited by finerenone?
a) Respiratory
b) Hepatic
c) Renal and cardiac
d) Central nervous system
Answer: c) Renal and cardiac
6. Major metabolic pathway of finerenone is:
a) CYP2D6
b) CYP3A4
c) Renal enzymes
d) Phase II conjugation
Answer: b) CYP3A4
7. Protein binding of finerenone is approximately:
a) 50%
b) 70%
c) 92%
d) 100%
Answer: c) 92%
8. Finerenone is preferable over spironolactone in:
a) Acute liver failure
b) Heart failure with fluid retention
c) CKD with diabetes
d) Hepatic encephalopathy
Answer: c) CKD with diabetes
9. Common adverse effect requiring monitoring:
a) Hypocalcemia
b) Hyperkalemia
c) Anemia
d) Leukopenia
Answer: b) Hyperkalemia
10. Finerenone lacks activity at which receptor?
a) Mineralocorticoid
b) Progesterone
c) Glucocorticoid
d) Estrogen
Answer: b) Progesterone
11. Its half-life supports:
a) Twice daily dosing
b) Once daily dosing
c) Weekly dosing
d) PRN dosing
Answer: b) Once daily dosing
12. One key trial for finerenone efficacy is:
a) EMPA-REG
b) FIDELIO-DKD
c) SOLVD
d) DAPA-HF
Answer: b) FIDELIO-DKD
13. Its antifibrotic action is critical in:
a) Muscle diseases
b) Hepatic cirrhosis
c) CKD progression
d) Retinal detachment
Answer: c) CKD progression
14. Unlike spironolactone, finerenone does not cause:
a) Hyperkalemia
b) Hypotension
c) Gynecomastia
d) Proteinuria
Answer: c) Gynecomastia
15. Primary route of elimination:
a) Biliary
b) Renal
c) Fecal and renal
d) Pulmonary
Answer: c) Fecal and renal
FAQs
1. How does finerenone differ from spironolactone?
Finerenone is nonsteroidal and highly selective for the MR, reducing off-target hormone-related side effects.
2. Can finerenone be used with ACE inhibitors or ARBs?
Yes, it is commonly added to existing RAAS blockade in CKD + T2DM patients, with potassium monitoring.
3. Is hyperkalemia still a concern?
Yes, but the risk is generally lower than that of steroidal MRAs.
4. What makes finerenone cardioprotective?
It reduces inflammation and fibrosis in the myocardium, decreasing the risk of heart failure events.
5. Is it useful in non-diabetic CKD?
Currently, its main indication is for CKD associated with T2DM. Trials are ongoing in broader populations.
References
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics, 13th Edition
- KD Tripathi. Essentials of Medical Pharmacology, 8th Edition
- DrugBank: Finerenone
- Frontiers in Medicine: Therapeutic Role of Finerenone
- Cardiovascular Diabetology: Finerenone in CKD and HFpEF
- FIDELIO-DKD Trial: Clinical efficacy data
- Nature Medicine: Finerenone’s cardiorenal effects
