Table of Contents
Introduction
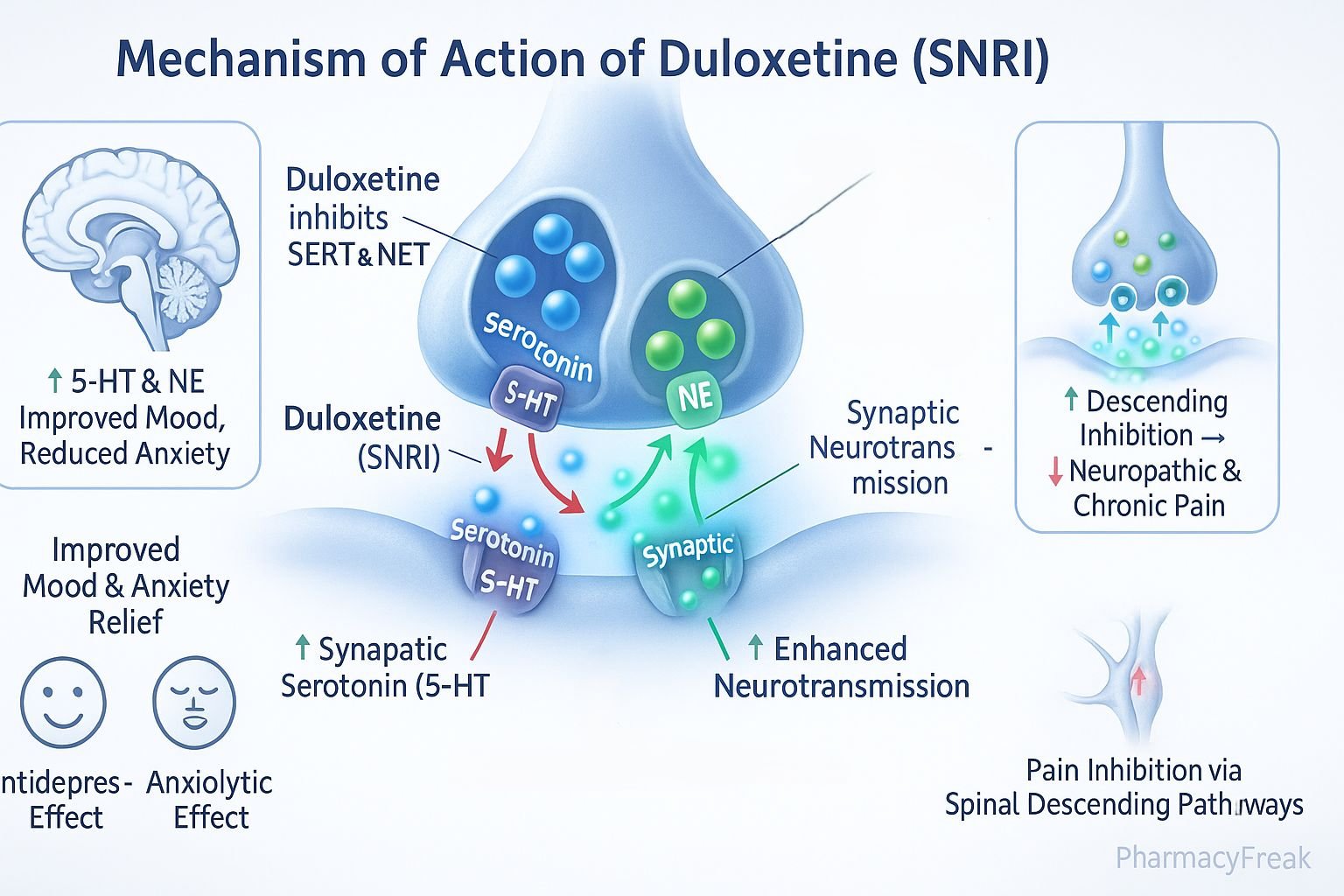
Duloxetine is a serotonin-norepinephrine reuptake inhibitor (SNRI) widely used in psychiatry and neurology. It is prescribed for major depressive disorder, generalized anxiety disorder, neuropathic pain, fibromyalgia, and chronic musculoskeletal pain. Mechanism of Action of Duloxetine centers on its ability to modulate central monoaminergic neurotransmission by inhibiting reuptake of serotonin and norepinephrine. This dual mechanism provides both antidepressant and analgesic effects, distinguishing it from selective serotonin reuptake inhibitors (SSRIs). Understanding its mechanism is critical for clinical use and optimizing patient therapy.
Mechanism of Action (Step-wise)
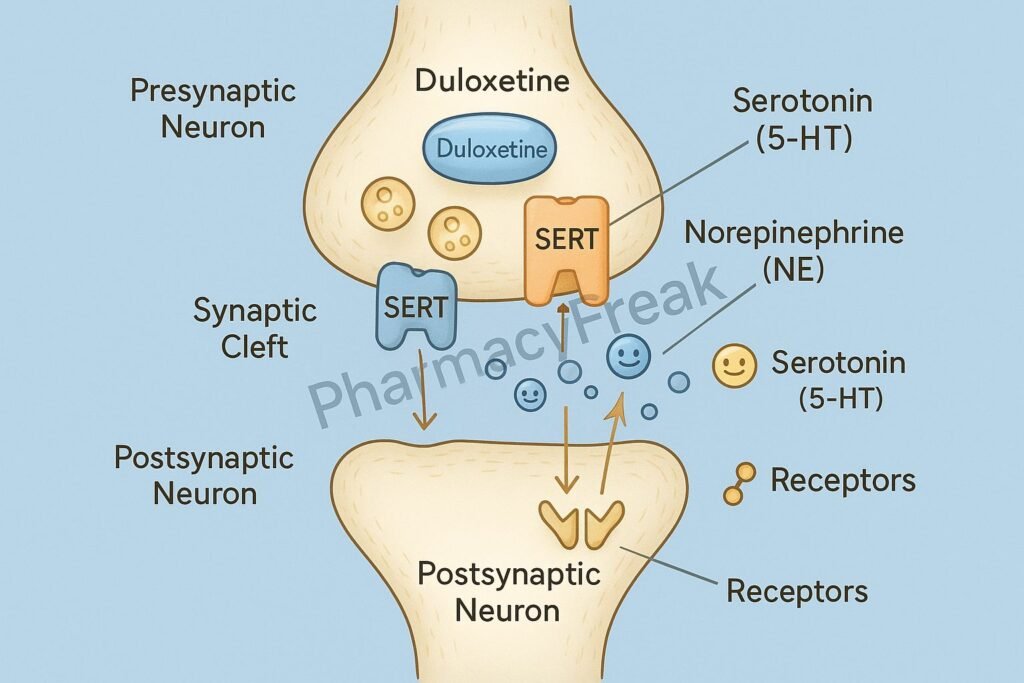
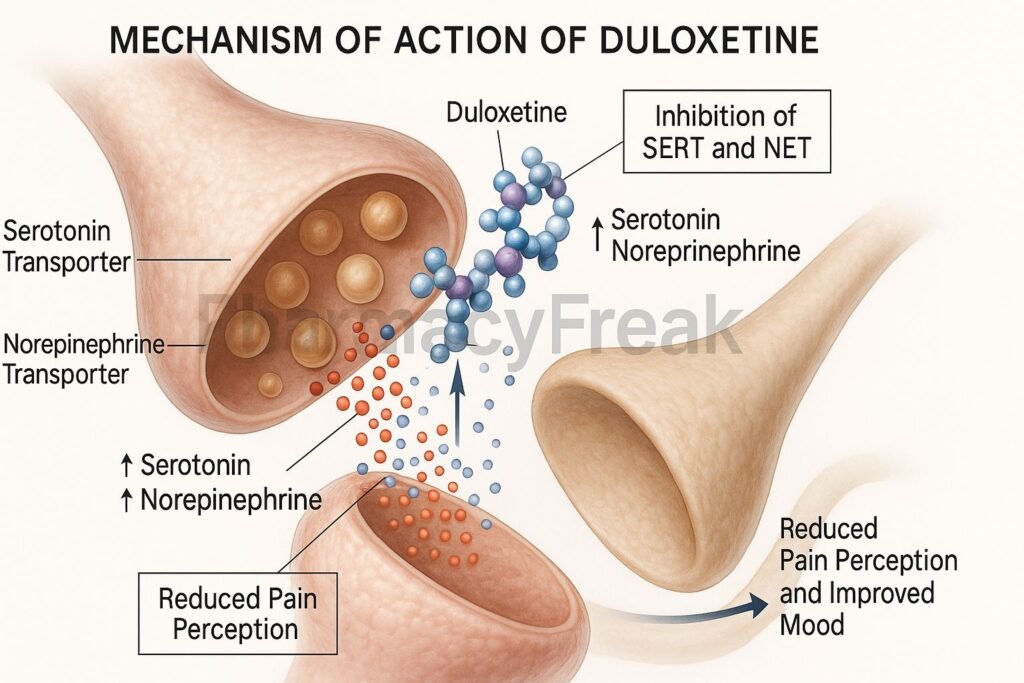
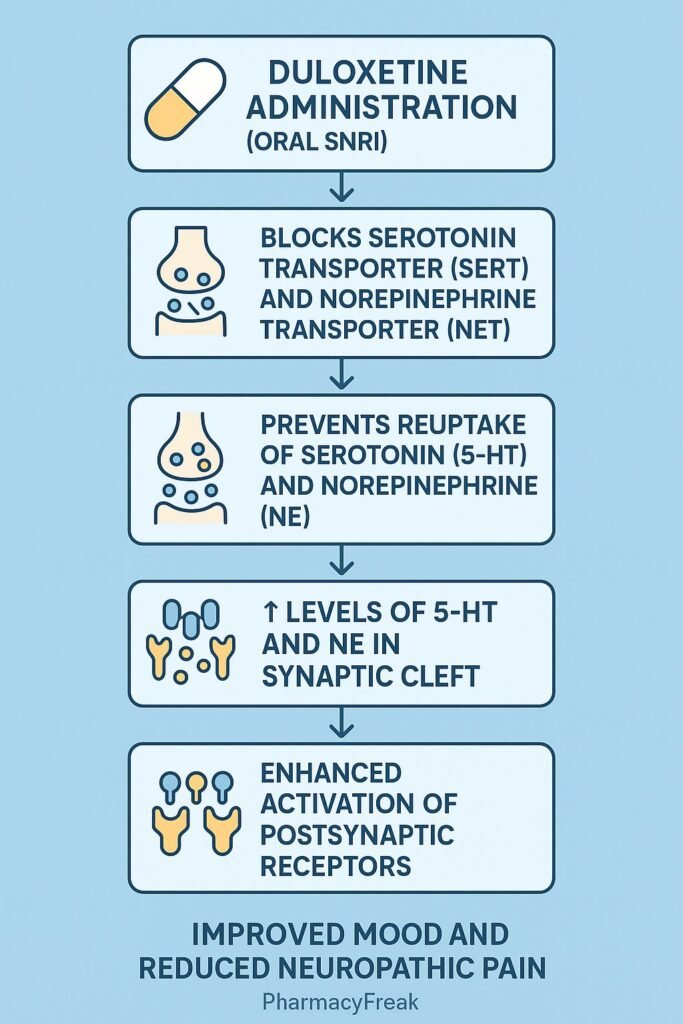
- Inhibition of Serotonin Transporter (SERT):
- Duloxetine blocks reuptake of serotonin into presynaptic neurons.
- This increases serotonin concentration in the synaptic cleft.
- Inhibition of Norepinephrine Transporter (NET):
- Duloxetine inhibits norepinephrine reuptake.
- Elevated norepinephrine enhances arousal, energy, and mood.
- Increased Neurotransmission:
- Higher serotonin and norepinephrine levels result in enhanced neurotransmission in the CNS.
- This improves mood and reduces anxiety.
- Modulation of Pain Pathways:
- Norepinephrine and serotonin modulate descending inhibitory pain pathways in the spinal cord.
- Duloxetine enhances these pathways, reducing pain perception.
- Overall Effect:
- Antidepressant action through serotonin and norepinephrine enhancement.
- Analgesic effect via modulation of central pain pathways.
Pharmacokinetics
- Absorption: Well absorbed orally; peak plasma levels within 6 hours.
- Distribution: Extensively protein-bound (~95%).
- Metabolism: Metabolized primarily in the liver by CYP1A2 and CYP2D6 enzymes.
- Excretion: Metabolites excreted in urine.
- Half-life: Approximately 12 hours, enabling once- or twice-daily dosing.
Clinical Uses
- Major depressive disorder (MDD).
- Generalized anxiety disorder (GAD).
- Diabetic peripheral neuropathic pain.
- Fibromyalgia.
- Chronic musculoskeletal pain.
- Off-label: stress urinary incontinence.
Adverse Effects
- Common: Nausea, dry mouth, constipation, somnolence, dizziness, sweating.
- Less common: Sexual dysfunction, hypertension, urinary retention.
- Serious: Hepatotoxicity, serotonin syndrome (especially with serotonergic drugs), suicidal ideation in young adults.
Comparative Analysis
| Feature | Duloxetine (SNRI) | SSRI (e.g., Sertraline) | TCA (e.g., Amitriptyline) |
|---|---|---|---|
| Mechanism | Inhibits serotonin & norepinephrine reuptake | Inhibits serotonin reuptake | Blocks serotonin & norepinephrine reuptake + anticholinergic |
| Analgesic effect | Yes | Minimal | Yes |
| Side effect profile | Moderate (GI, insomnia) | Fewer than TCAs | Anticholinergic, cardiotoxic |
| Weight effect | Neutral/slight loss | Neutral/weight gain | Weight gain common |
| Safety in overdose | Safer than TCAs | Very safe | Dangerous (arrhythmias) |
MCQs
1. Duloxetine belongs to which drug class?
a) SSRI
b) SNRI
c) TCA
d) MAOI
Answer: b) SNRI
2. The analgesic effect of duloxetine is due to:
a) Dopamine receptor blockade
b) Enhancement of descending inhibitory pain pathways
c) GABA receptor activation
d) NMDA receptor antagonism
Answer: b) Enhancement of descending inhibitory pain pathways
3. Which liver enzymes metabolize duloxetine?
a) CYP3A4 and CYP2C9
b) CYP1A2 and CYP2D6
c) CYP2C19 and CYP2E1
d) CYP4A and CYP2B6
Answer: b) CYP1A2 and CYP2D6
4. Which of the following is a common side effect of duloxetine?
a) Bradycardia
b) Constipation
c) Tinnitus
d) Alopecia
Answer: b) Constipation
5. Duloxetine is indicated in:
a) Parkinson’s disease
b) Fibromyalgia
c) Schizophrenia
d) Epilepsy
Answer: b) Fibromyalgia
6. What is the approximate half-life of duloxetine?
a) 2 hours
b) 6 hours
c) 12 hours
d) 24 hours
Answer: c) 12 hours
7. Duloxetine has a black box warning for:
a) Hypertension
b) Suicidal ideation in young adults
c) Nephrotoxicity
d) QT prolongation
Answer: b) Suicidal ideation in young adults
8. Which neurotransmitters are primarily affected by duloxetine?
a) Dopamine and norepinephrine
b) Serotonin and norepinephrine
c) GABA and glutamate
d) Acetylcholine and histamine
Answer: b) Serotonin and norepinephrine
9. Duloxetine is contraindicated in:
a) Hepatic impairment
b) Hypertension
c) Diabetes
d) Asthma
Answer: a) Hepatic impairment
10. Serotonin syndrome with duloxetine is more likely when combined with:
a) Beta-blockers
b) NSAIDs
c) Other serotonergic drugs
d) Anticholinergics
Answer: c) Other serotonergic drugs
FAQs
Q1. Is duloxetine the same as an SSRI?
No, duloxetine is an SNRI affecting both serotonin and norepinephrine, unlike SSRIs.
Q2. Can duloxetine be used for pain management?
Yes, it is approved for neuropathic pain, fibromyalgia, and chronic musculoskeletal pain.
Q3. Is dose adjustment required in renal impairment?
Yes, dose reduction is recommended in severe renal impairment.
Q4. How long does duloxetine take to show effect in depression?
Clinical improvement is usually seen in 2–4 weeks.
Q5. Can duloxetine cause withdrawal symptoms?
Yes, abrupt discontinuation may lead to dizziness, irritability, and flu-like symptoms.
Q6. Is duloxetine safe during pregnancy?
It is generally avoided unless benefits outweigh risks.
References
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics
- Stahl’s Essential Psychopharmacology
- Katzung Basic and Clinical Pharmacology
- FDA Prescribing Information for Duloxetine

