Table of Contents
Introduction
Carbonic anhydrase inhibitors (CAIs) are a class of diuretics and antiglaucoma drugs represented primarily by acetazolamide, dorzolamide, and brinzolamide. They reduce bicarbonate reabsorption in the kidney, decrease aqueous humor formation in the eye, and modulate cerebrospinal fluid (CSF) production.
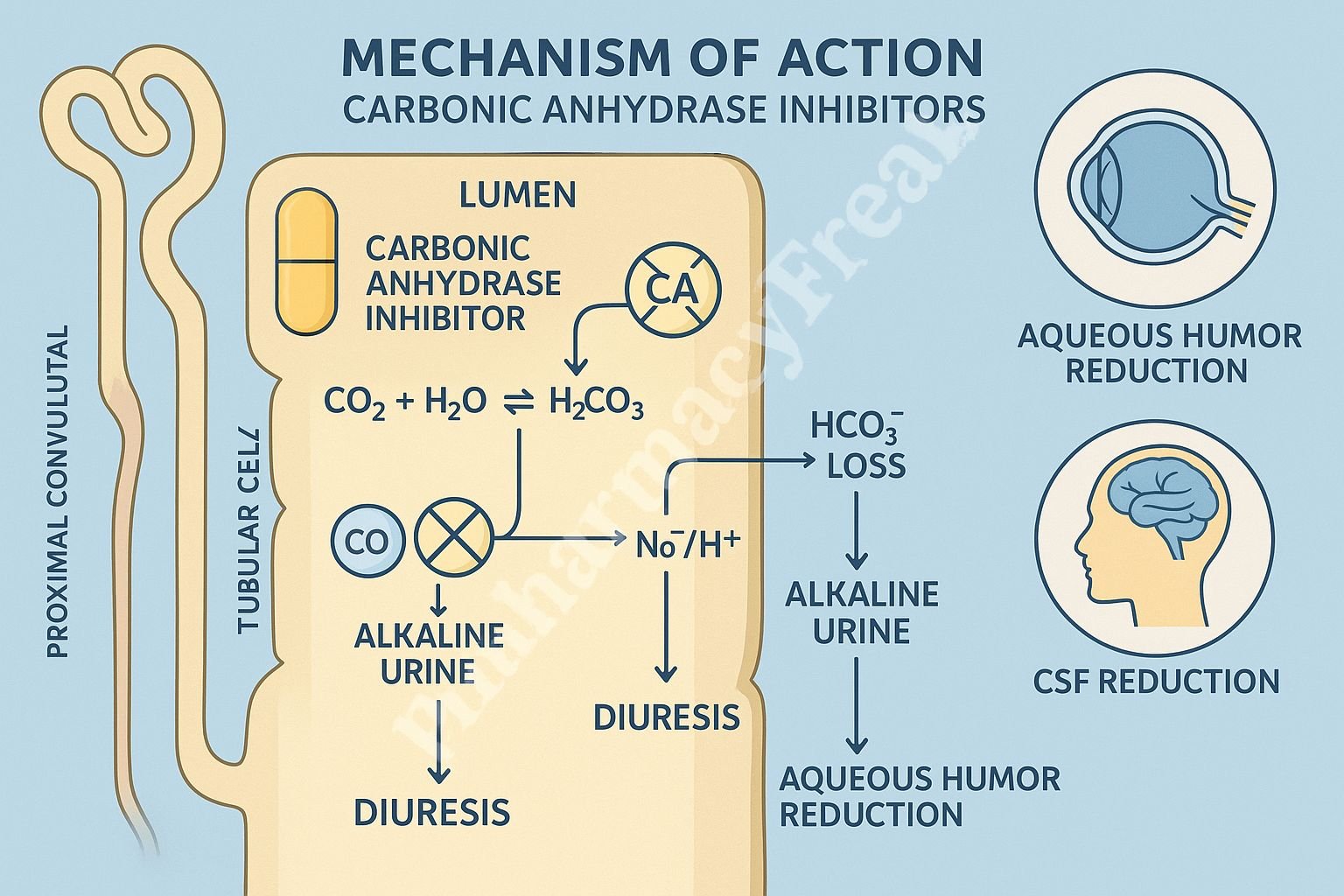
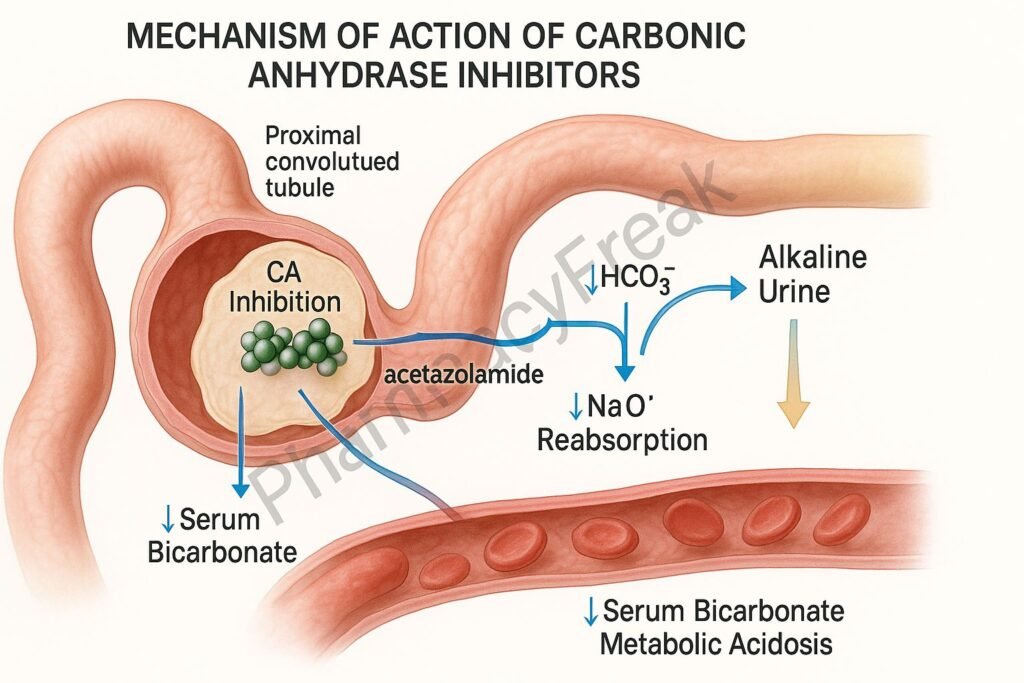
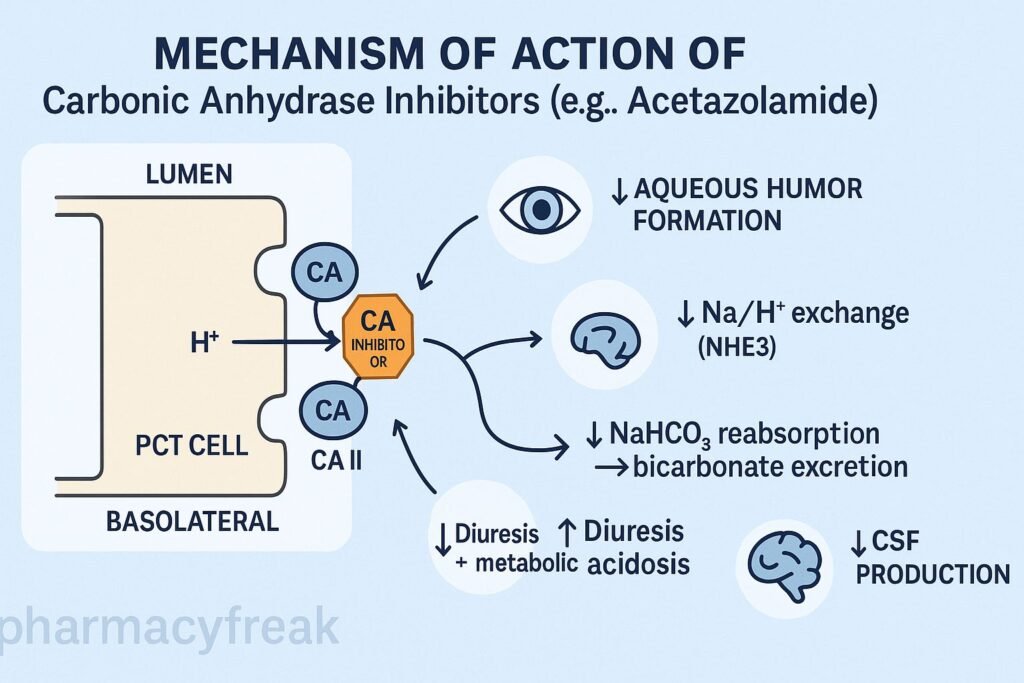
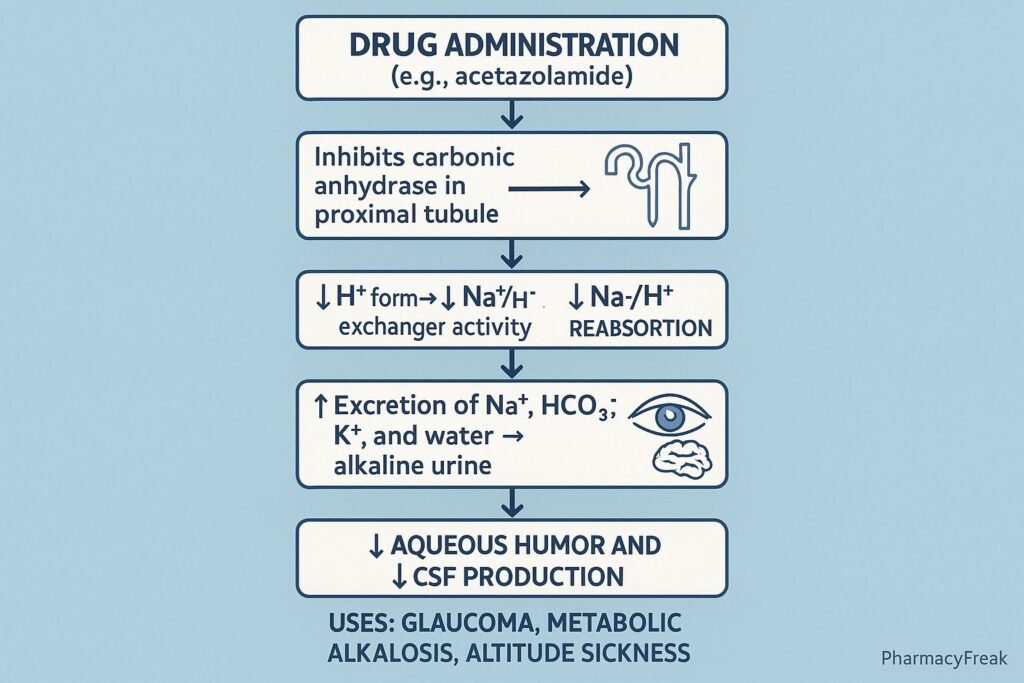
The Mechanism of Action of Carbonic Anhydrase Inhibitors centers on blocking the enzyme carbonic anhydrase (CA), primarily in the proximal convoluted tubule, leading to bicarbonate diuresis, reduced intraocular pressure, and decreased CSF synthesis.
Mechanism of Action (Step-wise)
1. Inhibition of Carbonic Anhydrase (CA-II and CA-IV) – Primary Mechanism
Carbonic anhydrase catalyzes:
- Hydration of CO₂ → H₂CO₃
- Dissociation of H₂CO₃ → H⁺ + HCO₃⁻
CAIs block this reaction.
Result:
- ↓ H⁺ availability inside tubular cells
- ↓ Na⁺/H⁺ exchange
- ↓ NaHCO₃ reabsorption
2. Increased Bicarbonate Excretion
Blocking CA prevents reabsorption of bicarbonate.
Effects:
- ↑ Urinary bicarbonate loss
- ↑ Alkaline urine
- ↓ Serum bicarbonate
- Metabolic acidosis
This limits long-term use as a diuretic.
3. Decreased Sodium and Water Reabsorption
Reduced H⁺ production leads to reduced Na⁺ reabsorption through Na⁺/H⁺ exchanger.
Effects:
- Mild natriuresis
- Mild diuresis
- Increased urine volume
CAIs are weak diuretics because most Na⁺ reabsorption occurs downstream.
4. Decreased Intraocular Pressure (IOP)
In the eye, carbonic anhydrase is essential for aqueous humor production.
CA inhibition →
- ↓ Bicarbonate formation
- ↓ Fluid secretion
- ↓ Aqueous humor volume
- ↓ Intraocular pressure
Topical CAIs (dorzolamide, brinzolamide) are used for glaucoma.
5. Decreased CSF Production
Carbonic anhydrase also regulates CSF formation in the choroid plexus.
Effects:
- ↓ CSF secretion
- Helpful in idiopathic intracranial hypertension (pseudotumor cerebri)
6. Promotes Respiratory Compensation
Metabolic acidosis induced by CAIs stimulates ventilation.
Results:
- ↑ Respiratory drive
- Useful in acute mountain sickness
7. Summary of Mechanism
| Mechanism | Effect |
|---|---|
| CA inhibition | ↓ HCO₃⁻ reabsorption |
| ↑ Bicarbonate excretion | Metabolic acidosis & alkaline urine |
| ↓ Na⁺ reabsorption | Mild diuresis |
| ↓ Aqueous humor | Lower intraocular pressure |
| ↓ CSF production | Useful in intracranial hypertension |
| ↑ Ventilation | Helps high-altitude sickness |
Pharmacokinetics
- Route: Oral (acetazolamide), topical (dorzolamide, brinzolamide)
- Onset: 1–2 hours (oral)
- Distribution: Well distributed; crosses placenta
- Elimination: Renal excretion
- Duration: 8–12 hours
Clinical Uses
- Glaucoma (topical/oral)
- Idiopathic intracranial hypertension
- Acute mountain sickness
- Epilepsy (adjunct)
- Metabolic alkalosis
- Periodic paralysis
- Mild diuresis
Adverse Effects
- Metabolic acidosis
- Hypokalemia
- Paresthesias
- Kidney stones (due to alkaline urine)
- Drowsiness
- Anorexia
- Sulfonamide hypersensitivity reactions
Contraindications
- Sulfonamide allergy
- Severe hepatic disease (risk of hyperammonemia)
- Hyponatremia or hypokalemia
- Renal failure
- COPD (acidosis may worsen respiratory status)
Comparative Analysis
| Feature | Acetazolamide | Dorzolamide | Brinzolamide |
|---|---|---|---|
| Route | Oral | Topical | Topical |
| Systemic effects | High | Low | Low |
| Use | Glaucoma, altitude | Glaucoma | Glaucoma |
| Diuresis | Mild | Minimal | Minimal |
MCQs
1. Carbonic anhydrase inhibitors act mainly in the:
a) Loop of Henle
b) Distal tubule
c) Proximal convoluted tubule
d) Collecting duct
Answer: c) Proximal convoluted tubule
2. A major biochemical consequence of CA inhibition is:
a) Respiratory alkalosis
b) Metabolic acidosis
c) Hypernatremia
d) Hypermagnesemia
Answer: b) Metabolic acidosis
3. CAIs lower intraocular pressure by decreasing:
a) Trabecular outflow
b) Aqueous humor formation
c) Uveoscleral flow
d) Lens accommodation
Answer: b) Aqueous humor formation
4. Acetazolamide helps altitude sickness by:
a) Reducing CSF pressure
b) Causing metabolic acidosis to stimulate ventilation
c) Causing respiratory depression
d) Increasing erythropoietin
Answer: b) Causing metabolic acidosis to stimulate ventilation
5. A common adverse effect is:
a) Myelosuppression
b) Kidney stones
c) Hypercalcemia
d) Hyperglycemia
Answer: b) Kidney stones
FAQs
Q1. Why are CAIs weak diuretics?
Because most sodium is reabsorbed downstream in the nephron.
Q2. Do CAIs cause acidosis or alkalosis?
They cause metabolic acidosis due to bicarbonate loss.
Q3. Which CAI is preferred for glaucoma?
Topical agents like dorzolamide and brinzolamide.
Q4. Why avoid CAIs in cirrhosis?
Risk of hyperammonemia due to impaired ammonia trapping.
Q5. Can CAIs be used long-term?
Limited by metabolic acidosis and risk of stones.
References
Goodman & Gilman’s Pharmacological Basis of Therapeutics
https://accesspharmacy.mhmedical.com/book.aspx?bookid=2189
Katzung: Basic and Clinical Pharmacology
https://accessmedicine.mhmedical.com/book.aspx?bookid=2464
Tripathi: Essentials of Medical Pharmacology
https://jaypeebrothers.com/
Harrison’s Principles of Internal Medicine
https://accessmedicine.mhmedical.com/book.aspx?bookid=2129


