Table of Contents
Introduction
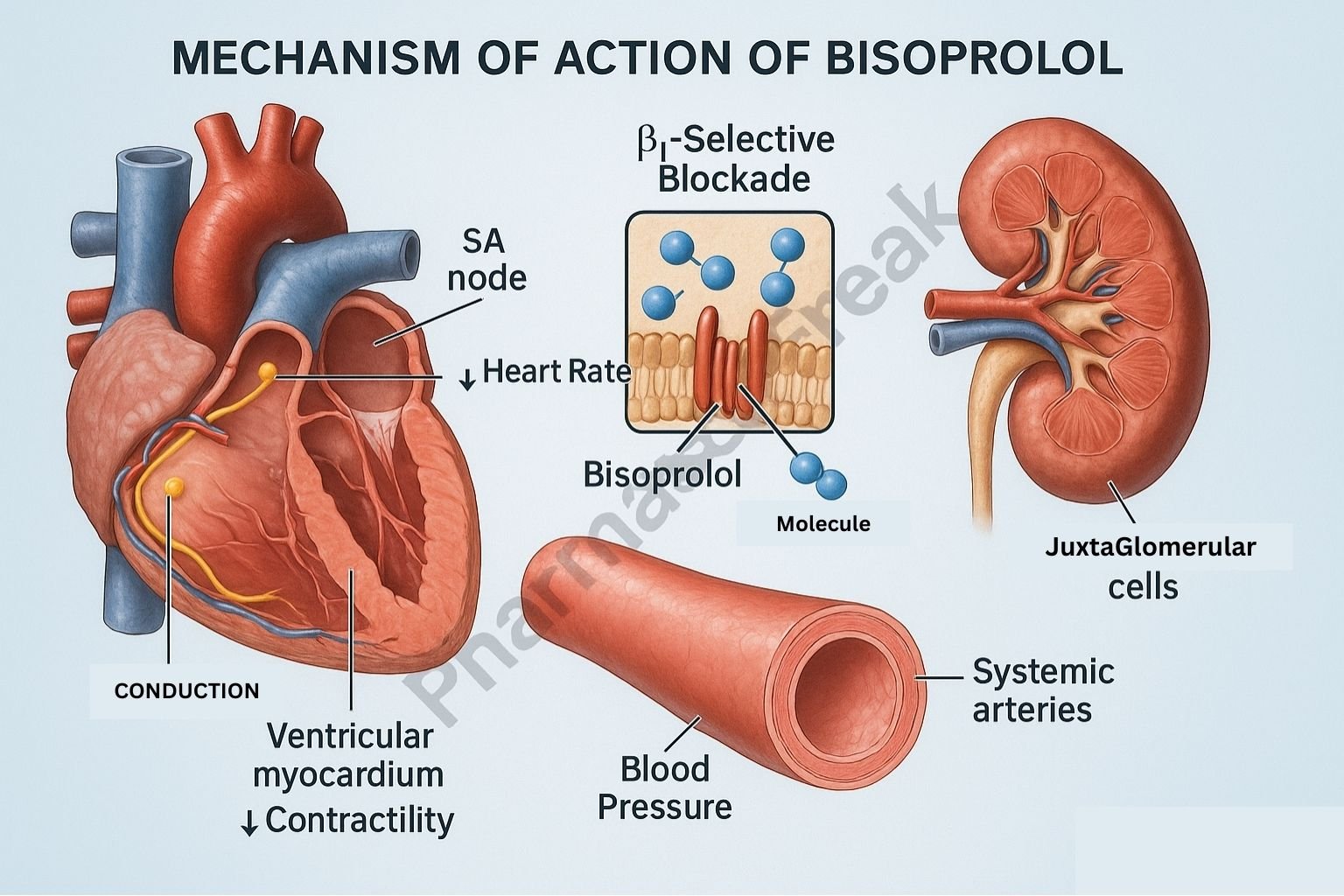
Bisoprolol is a highly selective beta-1 adrenergic receptor blocker used extensively in the management of hypertension, chronic heart failure, angina pectoris, and arrhythmias. As a cardioselective beta blocker, bisoprolol primarily targets beta-1 receptors in the heart, exerting strong negative chronotropic, inotropic, and dromotropic effects with minimal influence on beta-2 receptors in the lungs and vasculature.
Its high receptor selectivity and long half-life allow once-daily dosing and make it one of the most preferred beta-blockers in chronic cardiovascular therapy.



Mechanism of Action (Step-wise)
1. Selective Blockade of Beta-1 Adrenergic Receptors (Primary Mechanism)
Bisoprolol competitively inhibits beta-1 receptors in cardiac tissue.
This prevents activation by catecholamines (norepinephrine, epinephrine).
Effects:
- ↓ SA node firing → decreased heart rate (negative chronotropy)
- ↓ AV node conduction → reduced conduction velocity (negative dromotropy)
- ↓ Myocardial contractility → reduced cardiac workload (negative inotropy)
Overall effect: Lower myocardial oxygen demand and improved cardiac efficiency.
2. Suppression of Renin Release
Beta-1 receptors on juxtaglomerular cells in the kidneys stimulate renin release.
Bisoprolol blocks these receptors →
- ↓ Renin
- ↓ Angiotensin I → ↓ Angiotensin II
- ↓ Aldosterone secretion
Effect:
Reduced blood pressure through decreased vasoconstriction and reduced sodium/water retention.
3. Reduced Sympathetic Activity
Chronic bisoprolol therapy decreases sympathetic nervous system overactivity seen in heart failure and hypertension.
Effects:
- Stabilized heart rhythm
- Fewer arrhythmias
- Improved ventricular remodeling in heart failure
4. Improved Myocardial Oxygen Balance
By reducing HR and contractility:
- ↓ Oxygen demand
- ↑ Diastolic filling time
- Improved coronary perfusion
This is beneficial in stable angina and post-MI patients.
5. Hemodynamic Summary
| Site | Effect of Bisoprolol |
|---|---|
| Heart (SA node) | ↓ HR |
| AV node | ↓ Conduction |
| Myocardium | ↓ Contractility |
| Kidneys | ↓ Renin release |
| Systemic circulation | ↓ Blood pressure |
Pharmacokinetics
- Bioavailability: ~80–90%
- Absorption: Excellent oral absorption
- Metabolism: 50% hepatic, 50% renal
- Half-life: 10–12 hours
- Dosing: Typically once daily
Clinical Uses
- Hypertension
- Chronic heart failure (guideline-approved)
- Angina pectoris
- Atrial fibrillation rate control
- Supraventricular arrhythmias
- Post-MI long-term therapy
Adverse Effects
- Bradycardia
- Hypotension
- Fatigue
- Cold extremities
- Dizziness
- Depression (rare)
- Bronchospasm (rare due to high selectivity)
Contraindications
- Severe bradycardia
- AV block (2nd/3rd degree)
- Decompensated heart failure
- Severe asthma (use caution)
- Cardiogenic shock
Comparative Analysis
| Feature | Bisoprolol | Metoprolol | Propranolol |
|---|---|---|---|
| Selectivity | Highly β1 selective | β1 selective | Non-selective |
| Half-life | Long (QD dosing) | Shorter | Shorter |
| Heart failure use | Strong evidence | Strong evidence | Not preferred |
| Bronchospasm risk | Lowest | Moderate | High |
MCQs
1. Bisoprolol primarily blocks which receptor?
a) Beta-2
b) Alpha-1
c) Beta-1
d) M2
Answer: c) Beta-1
2. Reduction of blood pressure by bisoprolol is partly due to:
a) Increased renin release
b) Decreased angiotensin II levels
c) Increased aldosterone
d) Increased cardiac output
Answer: b) Decreased angiotensin II levels
3. Bisoprolol decreases myocardial oxygen demand by:
a) Increasing SV
b) Increasing HR
c) Decreasing contractility
d) Increasing AV conduction
Answer: c) Decreasing contractility
4. Bisoprolol is preferred in:
a) Acute asthma attack
b) Chronic heart failure
c) Hyperthyroid ophthalmopathy
d) Shock
Answer: b) Chronic heart failure
5. A major adverse effect of bisoprolol is:
a) Hyperkalemia
b) Bradycardia
c) Hyperthyroidism
d) Increased GI motility
Answer: b) Bradycardia
FAQs
Q1. Is bisoprolol safe for patients with asthma?
Generally safer than non-selective beta blockers, but caution is advised.
Q2. Can bisoprolol be stopped abruptly?
No—sudden withdrawal may cause rebound tachycardia or hypertension.
Q3. Is bisoprolol good for heart failure?
Yes—one of the three beta-blockers with proven mortality benefit.
Q4. Does bisoprolol cause weight gain?
Rarely; fluid retention may occur but is uncommon.
Q5. Why choose bisoprolol over metoprolol?
Higher β1 selectivity, longer action, smoother BP/HR control.
References
Goodman and Gilman – Pharmacological Basis of Therapeutics
Katzung – Basic and Clinical Pharmacology
Tripathi – Essentials of Medical Pharmacology
Harrison – Principles of Internal Medicine


