Table of Contents
🔍 Introduction
Escitalopram is a widely prescribed antidepressant belonging to the class of Selective Serotonin Reuptake Inhibitors (SSRIs). It is the S-enantiomer of citalopram and is considered one of the most selective SSRIs available.
Escitalopram is mainly used to treat:
- Major depressive disorder (MDD)
- Generalized anxiety disorder (GAD)
- Panic disorder and social anxiety disorder (off-label)
Due to its clean pharmacological profile and importance in psychiatry, Escitalopram is frequently tested in exams like GPAT, NEET-PG, NCLEX, and taught in PharmD, MBBS, and B.Pharm curricula.
🧬 Stepwise Mechanism of Action of Escitalopram
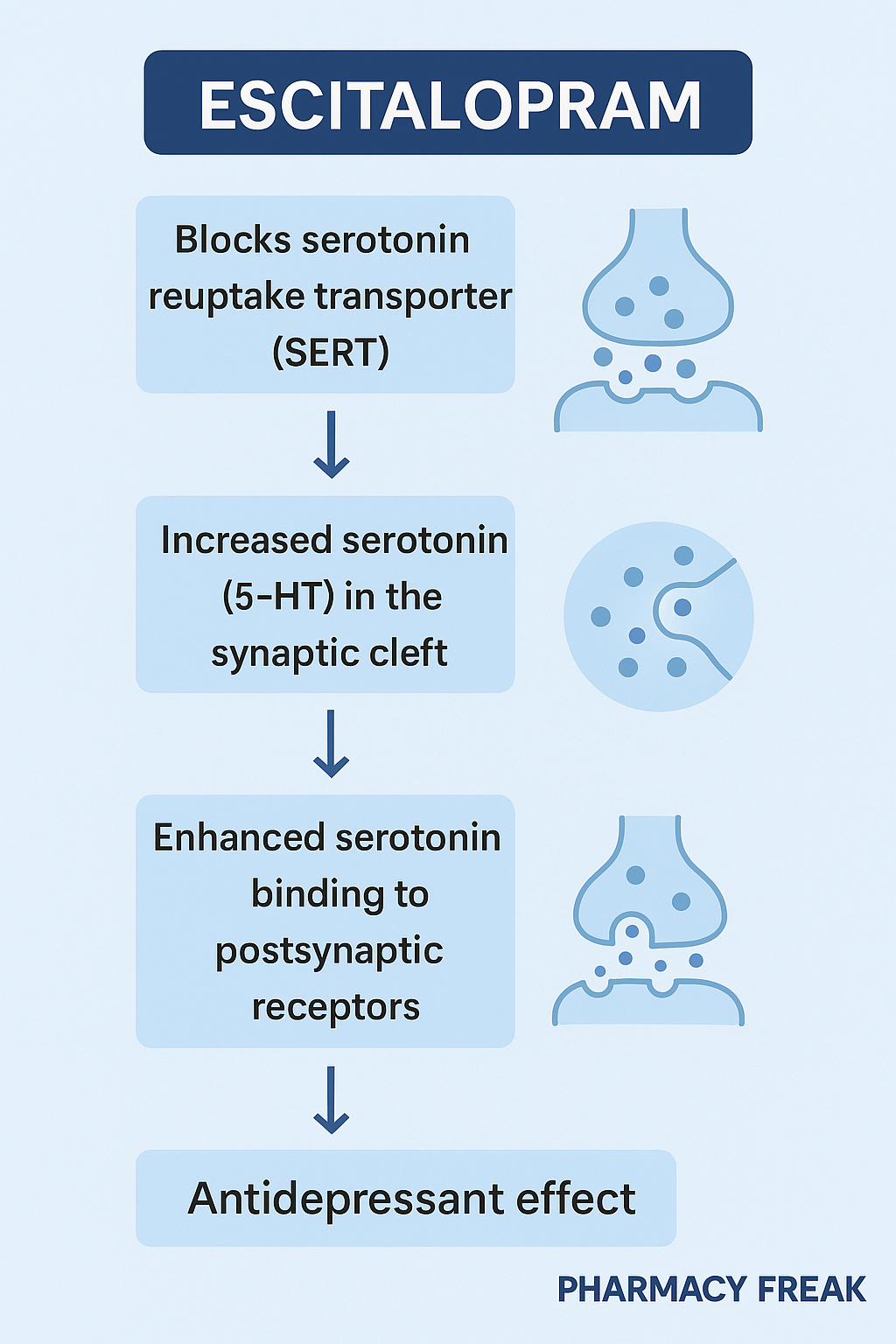
- Selective Inhibition of Serotonin Transporter (SERT):
Escitalopram binds with high affinity to the serotonin reuptake transporter (SERT) on presynaptic neurons, preventing reabsorption of serotonin (5-HT) from the synaptic cleft. - Increased Serotonin Levels in Synaptic Cleft:
Blockade of SERT results in elevated extracellular serotonin levels, especially in brain regions like the limbic system and prefrontal cortex. - Prolonged Serotonin Signaling:
The increased availability of serotonin leads to enhanced serotonergic neurotransmission, which contributes to mood elevation and anxiety reduction. - Delayed Onset Due to Receptor Desensitization:
Therapeutic effects usually take 2–4 weeks due to downregulation/desensitization of 5-HT1A autoreceptors, which normally limit serotonin release. - High Selectivity for SERT:
Unlike other SSRIs, Escitalopram shows minimal affinity for norepinephrine and dopamine transporters or histaminic, muscarinic, and alpha receptors → fewer side effects.
🧪 Pharmacokinetic Parameters of Escitalopram
| Parameter | Value |
|---|---|
| Bioavailability | ~80% (oral) |
| Onset of Action | 1–4 weeks (clinical effect) |
| Half-life | ~27–32 hours |
| Protein Binding | ~56% |
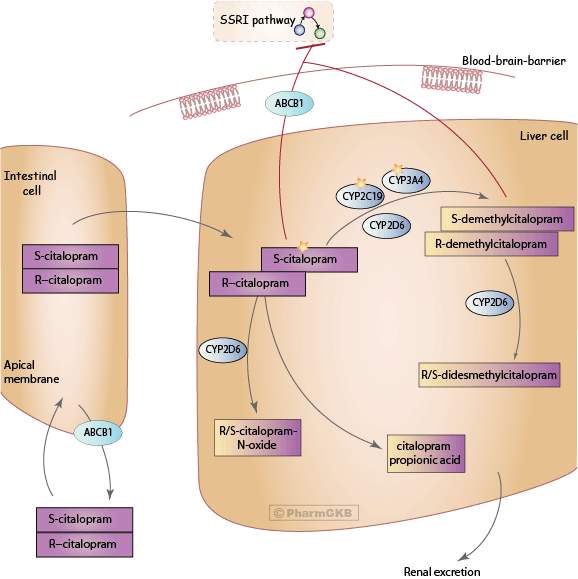
| Metabolism | Liver (via CYP2C19, CYP2D6, CYP3A4) |
| Excretion | Renal and hepatic routes (mostly metabolites) |
💊 Clinical Uses of Escitalopram
- Major Depressive Disorder (MDD)
- Generalized Anxiety Disorder (GAD)
- Panic disorder (off-label)
- Obsessive-compulsive disorder (OCD, off-label)
- Social anxiety disorder
- Premenstrual dysphoric disorder (PMDD, off-label)
⚠️ Adverse Effects of Escitalopram
- Nausea, insomnia, dry mouth
- Headache, dizziness
- Sexual dysfunction (common with SSRIs)
- Increased risk of suicidal ideation in adolescents
- QT interval prolongation at high doses
- Serotonin syndrome (when combined with MAOIs or serotonergic drugs)
🔬 Comparative Analysis: Escitalopram vs Fluoxetine
| Feature | Escitalopram | Fluoxetine |
|---|---|---|
| Class | SSRI | SSRI |
| Half-life | ~27–32 hours | ~2–4 days (long-acting) |
| Onset of action | 1–2 weeks | 2–4 weeks |
| QT Prolongation risk | Moderate at high doses | Low |
| Drug interactions | Fewer | More (inhibits CYP2D6) |
| Use in pregnancy | Category C | Category C |
📝 Practice MCQs
Q1. Escitalopram acts by:
A. Inhibiting MAO-A
B. Blocking dopamine receptors
C. Selectively inhibiting serotonin reuptake ✅
D. Enhancing norepinephrine release
Q2. Which transporter does Escitalopram bind to?
A. Dopamine transporter
B. Norepinephrine transporter
C. Serotonin transporter (SERT) ✅
D. GABA transporter
Q3. Clinical response to Escitalopram typically begins in:
A. 12 hours
B. 1–2 days
C. 2–4 weeks ✅
D. Immediately
Q4. Which of the following is a common side effect of Escitalopram?
A. Hepatotoxicity
B. Sexual dysfunction ✅
C. Alopecia
D. Visual hallucinations
Q5. Escitalopram is contraindicated with:
A. NSAIDs
B. MAO inhibitors ✅
C. Antacids
D. Paracetamol
Q6. Escitalopram is metabolized by which cytochrome enzymes?
A. CYP1A2
B. CYP2C19, CYP3A4, CYP2D6 ✅
C. CYP2E1
D. CYP7A1
Q7. Which of the following SSRIs has the highest selectivity for serotonin transporters?
A. Sertraline
B. Paroxetine
C. Escitalopram ✅
D. Fluoxetine
Q8. A rare but serious complication of combining Escitalopram with serotonergic drugs is:
A. Neuroleptic malignant syndrome
B. Serotonin syndrome ✅
C. Hypertensive crisis
D. Malignant hyperthermia
Q9. The action of Escitalopram leads to which of the following clinical effects?
A. Antipsychotic effect
B. Mood stabilization
C. Antianxiety and antidepressant effects ✅
D. Sedation only
Q10. Which of the following is least likely with Escitalopram use?
A. QT prolongation
B. Nausea
C. Sedation ✅
D. Delayed ejaculation
❓FAQs
Q1: Can Escitalopram be used in pregnancy?
Generally avoided unless benefits outweigh risks (Pregnancy Category C).
Q2: How long should Escitalopram be taken for depression?
Minimum of 6 months after symptom resolution; long-term use depends on clinical need.
Q3: Is dose adjustment needed in renal or hepatic impairment?
Yes. Start with lower doses in elderly, liver impairment, or renal dysfunction.
Q4: What is the major advantage of Escitalopram over older antidepressants?
Greater selectivity for SERT → fewer side effects and better tolerability.
📚 References
- KD Tripathi – Essentials of Medical Pharmacology, 8th Edition
- Sparsh Gupta – Review of Pharmacology
- Goodman & Gilman – The Pharmacological Basis of Therapeutics

