Table of Contents
Introduction
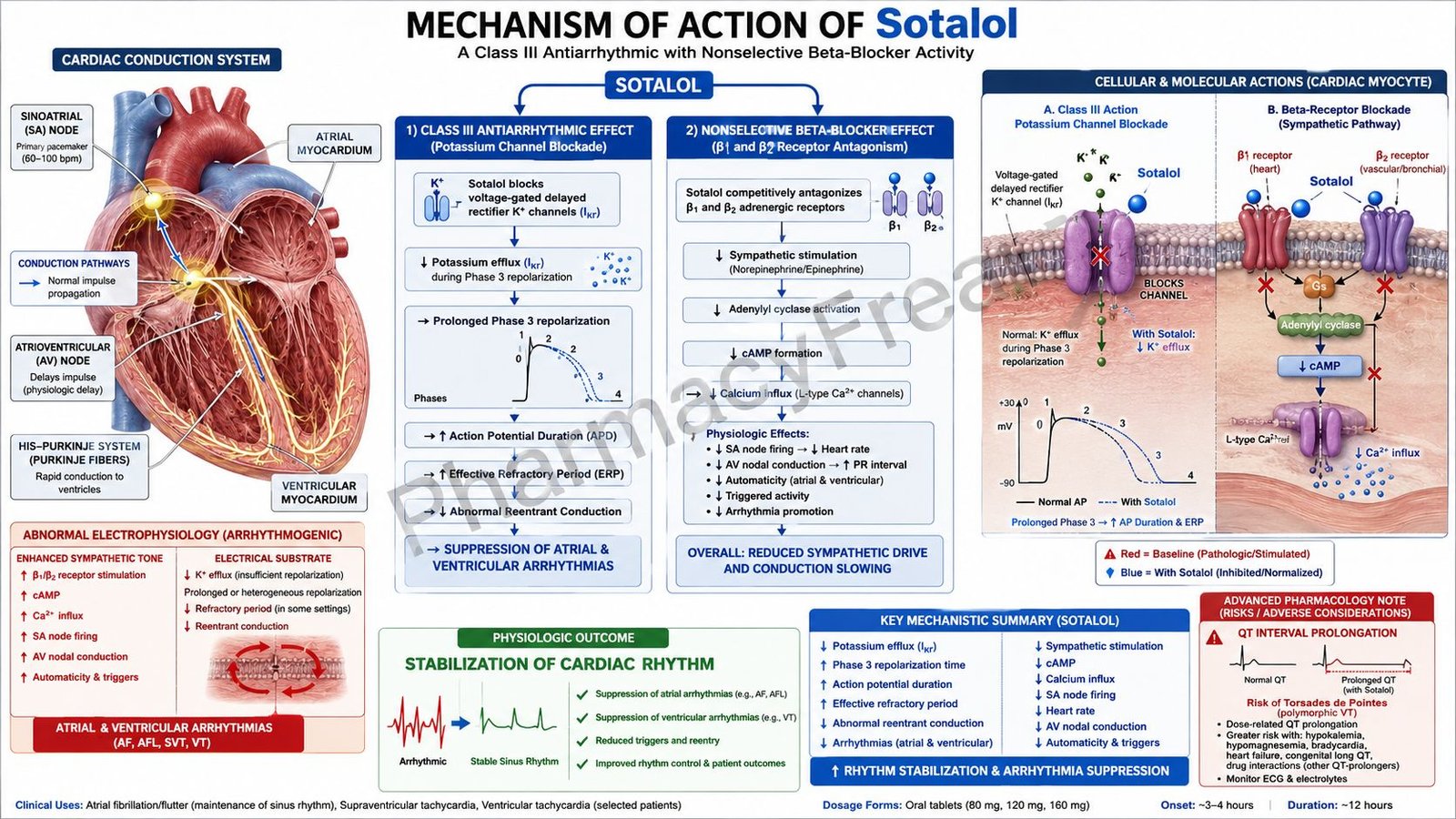
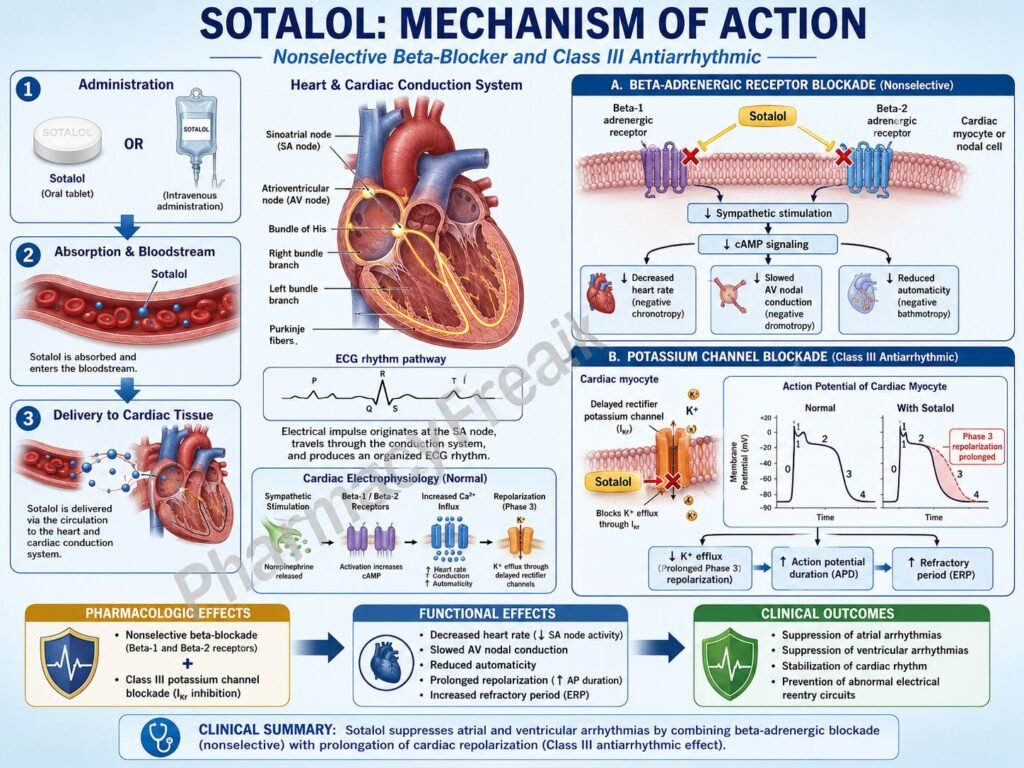
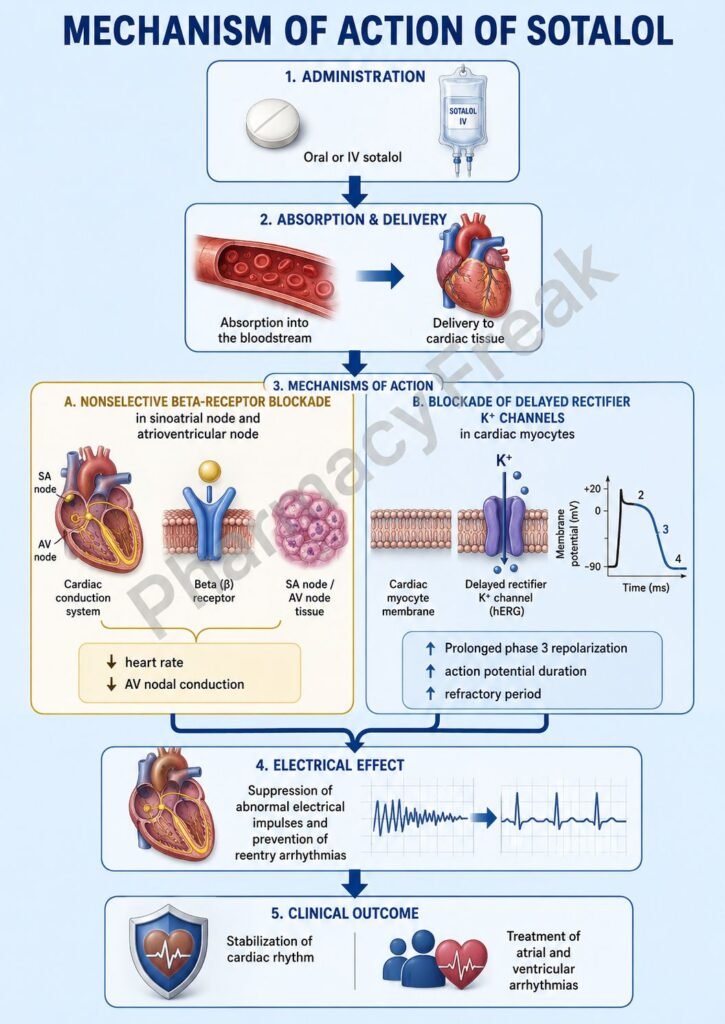
Sotalol is an antiarrhythmic medication with both nonselective β-adrenergic blocking activity and potassium channel-blocking properties. It is classified mainly as a Class III antiarrhythmic drug but also exhibits Class II β-blocker effects. Sotalol is used in ventricular arrhythmias and atrial fibrillation to maintain normal cardiac rhythm.
Mechanism of Action (Step-wise)
- Sotalol nonselectively blocks β1 and β2 adrenergic receptors in the heart.
- β1 receptor blockade decreases sympathetic stimulation of the sinoatrial (SA) node.
- Heart rate and automaticity decrease.
- Atrioventricular (AV) nodal conduction slows.
- Myocardial oxygen demand decreases because of reduced heart rate and contractility.
- Sotalol also blocks delayed rectifier potassium channels (IKr) in cardiac tissue.
- Potassium channel blockade prolongs phase 3 repolarization of the cardiac action potential.
- Action potential duration and effective refractory period increase in atrial and ventricular myocardium.
- Prolonged refractory periods suppress reentry circuits responsible for tachyarrhythmias.
- QT interval on ECG becomes prolonged because of delayed repolarization.
- The overall effect is suppression of abnormal cardiac rhythms and maintenance of sinus rhythm.
A key exam point is that sotalol combines nonselective β blockade with Class III potassium channel blockade to prolong cardiac repolarization.
Pharmacokinetics
Sotalol is administered orally and is well absorbed. Unlike many antiarrhythmics, it undergoes minimal hepatic metabolism and is excreted mainly unchanged through the kidneys. Dose adjustment is required in renal impairment.
Clinical Uses
Sotalol is used in atrial fibrillation, atrial flutter, supraventricular tachycardia, and life-threatening ventricular arrhythmias such as ventricular tachycardia.
Adverse Effects
Common adverse effects include bradycardia, fatigue, dizziness, hypotension, and bronchospasm due to β2 blockade. A major serious adverse effect is torsades de pointes caused by excessive QT prolongation.
Comparative Analysis
| Feature | Sotalol | Amiodarone | Metoprolol |
|---|---|---|---|
| Drug class | Class III + β blocker | Class III antiarrhythmic | β1 blocker |
| Potassium channel blockade | Yes | Yes | No |
| β blockade | Nonselective | Mild | Selective β1 |
| QT prolongation | Significant | Moderate | Minimal |
| Torsades risk | Higher | Lower | Minimal |
| Bronchospasm risk | Present | Minimal | Lower |
Sotalol differs from metoprolol because it additionally prolongs cardiac repolarization through potassium channel blockade. Compared with amiodarone, sotalol has a higher risk of torsades de pointes.
MCQs
- Sotalol belongs mainly to which antiarrhythmic class?
a) Class I
b) Class II
c) Class III
d) Class IV
Answer: c) Class III
- Sotalol blocks which cardiac channels?
a) Sodium channels only
b) Potassium channels
c) Calcium channels only
d) Chloride channels
Answer: b) Potassium channels
- Sotalol also acts as a:
a) Calcium channel blocker
b) Nonselective β blocker
c) α agonist
d) Cholinergic agonist
Answer: b) Nonselective β blocker
- Potassium channel blockade prolongs which phase of the cardiac action potential?
a) Phase 0
b) Phase 1
c) Phase 2
d) Phase 3
Answer: d) Phase 3
- Sotalol prolongs the:
a) PR interval only
b) QT interval
c) ST depression only
d) P wave amplitude only
Answer: b) QT interval
- Sotalol suppresses arrhythmias mainly by increasing:
a) Automaticity
b) Refractory period
c) Calcium influx only
d) Histamine release
Answer: b) Refractory period
- Sotalol is commonly used in:
a) Atrial fibrillation
b) Asthma
c) Diabetes mellitus
d) Peptic ulcer disease
Answer: a) Atrial fibrillation
- A serious adverse effect of sotalol is:
a) Torsades de pointes
b) Hypercalcemia
c) Cataracts
d) Polycythemia
Answer: a) Torsades de pointes
- β2 blockade by sotalol may cause:
a) Bronchodilation
b) Bronchospasm
c) Hyperglycemia
d) Vasodilation only
Answer: b) Bronchospasm
- Sotalol decreases heart rate by blocking:
a) β1 receptors
b) Histamine receptors
c) Muscarinic receptors
d) Dopamine receptors
Answer: a) β1 receptors
- Sotalol is eliminated mainly through the:
a) Liver
b) Kidneys
c) Lungs
d) Skin
Answer: b) Kidneys
- Compared with metoprolol, sotalol additionally:
a) Blocks potassium channels
b) Stimulates β receptors
c) Inhibits calcium channels only
d) Causes vasoconstriction
Answer: a) Blocks potassium channels
FAQs
What is the mechanism of action of sotalol?
Sotalol blocks β receptors and cardiac potassium channels, prolonging repolarization and refractory periods.
Why is sotalol classified as a Class III antiarrhythmic?
Because it prolongs phase 3 repolarization through potassium channel blockade.
What arrhythmias are treated with sotalol?
Atrial fibrillation, atrial flutter, and ventricular arrhythmias.
What is a major serious side effect of sotalol?
Torsades de pointes due to QT prolongation.
Why can sotalol cause bronchospasm?
Because it blocks β2 receptors in bronchial smooth muscle.
How does sotalol differ from metoprolol?
Sotalol also blocks potassium channels and prolongs cardiac repolarization.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics – Antiarrhythmic Drugs
https://accessmedicine.mhmedical.com/book.aspx?bookid=3191
Katzung: Basic and Clinical Pharmacology – Antiarrhythmic Agents
https://accessmedicine.mhmedical.com/content.aspx?bookid=3382
Tripathi: Essentials of Medical Pharmacology – Antiarrhythmic Drugs
https://www.jaypeedigital.com
Harrison’s Principles of Internal Medicine – Cardiac Arrhythmias
https://accessmedicine.mhmedical.com

