Table of Contents
Introduction
Repaglinide is an oral antidiabetic drug belonging to the meglitinide class. It is primarily used in type 2 diabetes mellitus to control postprandial blood glucose levels. Repaglinide stimulates rapid insulin secretion from pancreatic β-cells by closing ATP-sensitive potassium channels, thereby improving glucose control after meals.
Mechanism of Action (Step-wise)
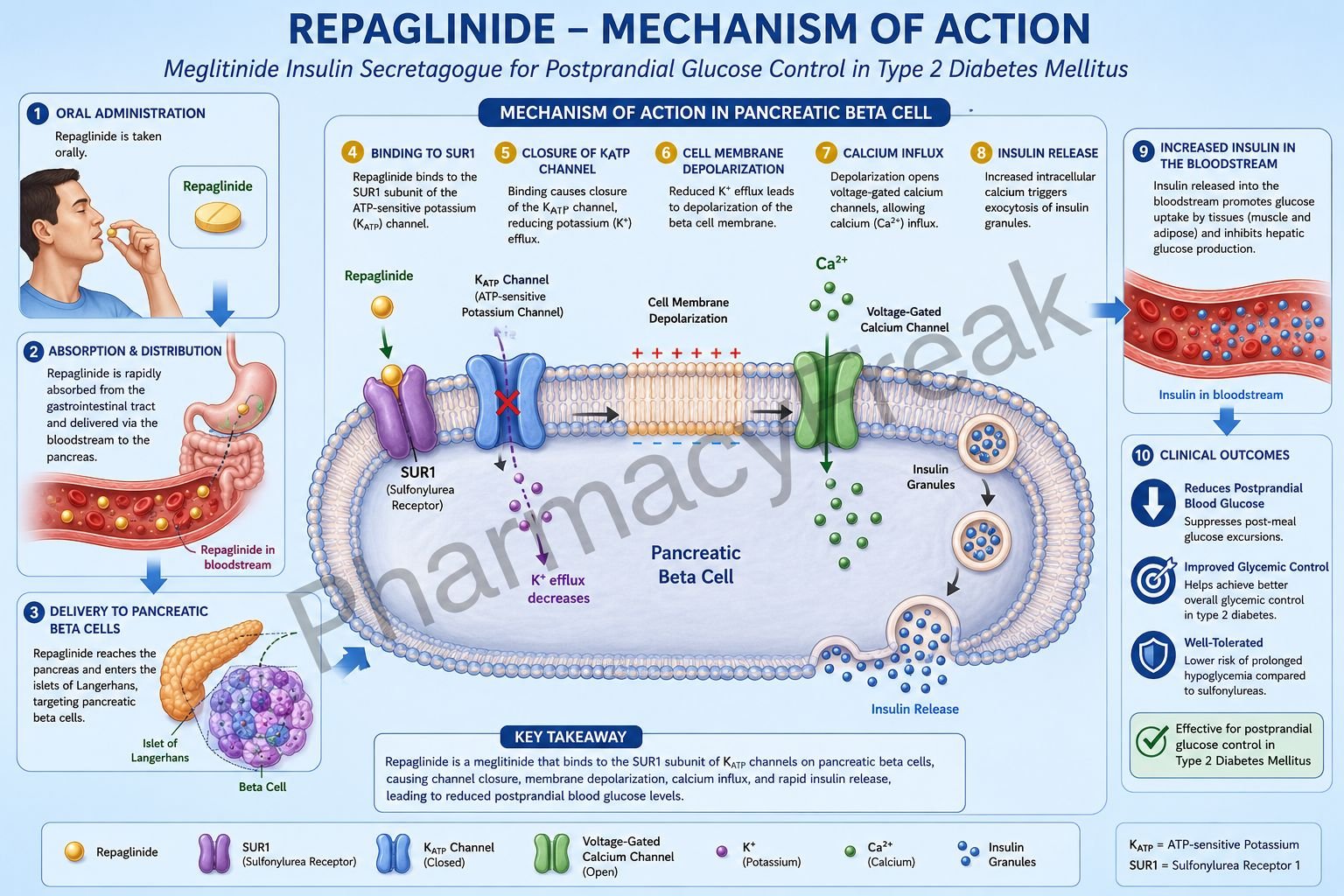
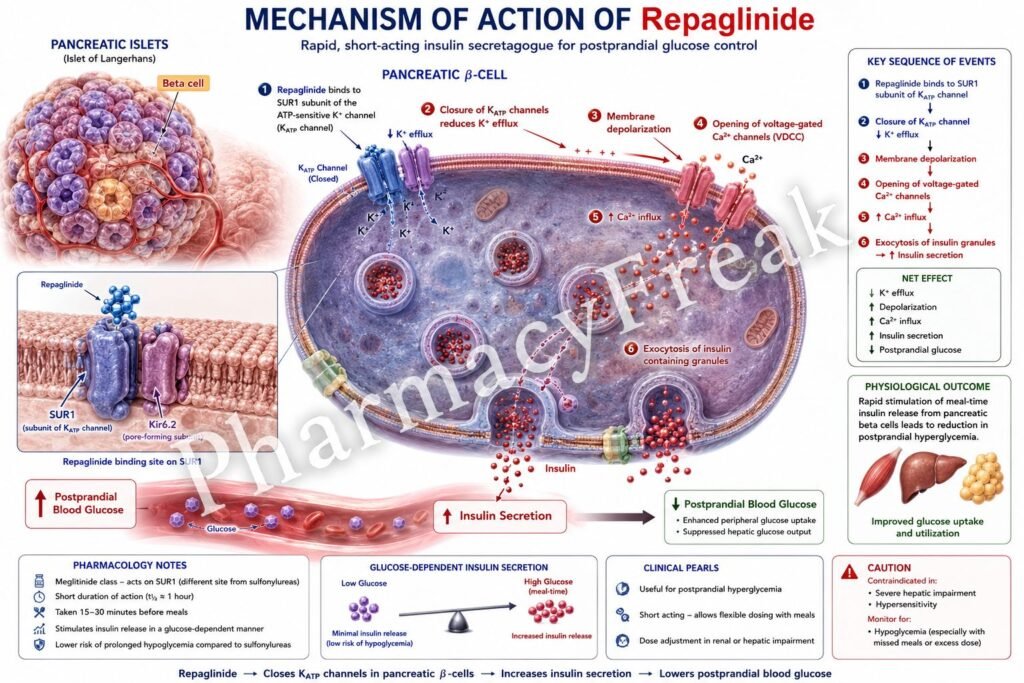
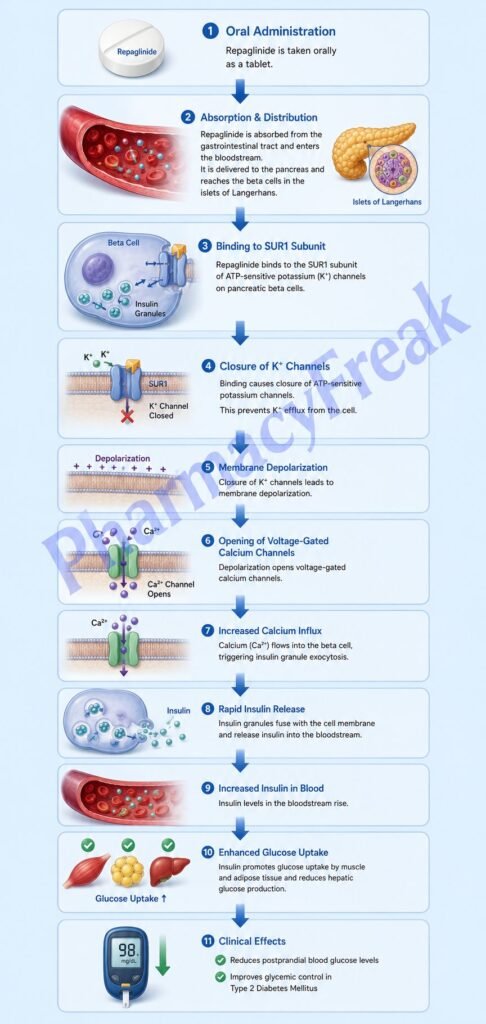
- Repaglinide acts on pancreatic β-cells in the islets of Langerhans.
- It binds to ATP-sensitive potassium (KATP) channels on β-cell membranes.
- Specifically, it interacts with the sulfonylurea receptor-1 (SUR1) subunit of the KATP channel.
- Binding closes potassium channels and prevents potassium efflux.
- Reduced potassium efflux causes depolarization of the β-cell membrane.
- Membrane depolarization opens voltage-gated calcium channels.
- Calcium influx into β-cells increases intracellular calcium concentration.
- Increased intracellular calcium triggers exocytosis of insulin-containing granules.
- Insulin secretion increases rapidly after administration.
- Released insulin promotes glucose uptake by tissues and lowers blood glucose levels.
- Repaglinide mainly targets postprandial hyperglycemia because of its rapid onset and short duration.
- The overall effect is improved glycemic control in type 2 diabetes mellitus.
A key exam point is that repaglinide stimulates insulin release by closing ATP-sensitive potassium channels in pancreatic β-cells.
Pharmacokinetics
Repaglinide is administered orally and is rapidly absorbed. It has a quick onset and short duration of action, making it suitable for premeal dosing. The drug is metabolized mainly in the liver through CYP3A4 and CYP2C8 pathways. Excretion occurs mainly via bile.
Clinical Uses
Repaglinide is used in type 2 diabetes mellitus, especially for controlling postprandial glucose excursions. It is often prescribed in patients with irregular meal schedules because doses can be adjusted according to meals.
Adverse Effects
The most common adverse effect is hypoglycemia. Weight gain may also occur due to increased insulin secretion. Compared with sulfonylureas, hypoglycemia risk may be somewhat lower because of the shorter duration of action.
Comparative Analysis
| Feature | Repaglinide | Glibenclamide | Metformin |
|---|---|---|---|
| Drug class | Meglitinide | Sulfonylurea | Biguanide |
| Main mechanism | Stimulates insulin secretion | Stimulates insulin secretion | Decreases hepatic glucose production |
| Target | KATP channels | KATP channels | Liver |
| Duration | Short | Longer | Moderate |
| Main glucose control | Postprandial | Fasting + postprandial | Fasting |
| Hypoglycemia risk | Moderate | Higher | Minimal |
Repaglinide differs from sulfonylureas by having faster onset and shorter duration of action. Compared with metformin, it directly increases insulin secretion rather than improving insulin sensitivity.
MCQs
- Repaglinide belongs to which drug class?
a) Biguanides
b) Meglitinides
c) Thiazolidinediones
d) DPP-4 inhibitors
Answer: b) Meglitinides
- Repaglinide acts primarily on:
a) Hepatocytes
b) Pancreatic β-cells
c) Skeletal muscle only
d) Renal tubules
Answer: b) Pancreatic β-cells
- Repaglinide binds to which channel?
a) Sodium channel
b) ATP-sensitive potassium channel
c) Calcium channel only
d) Chloride channel
Answer: b) ATP-sensitive potassium channel
- Closure of KATP channels causes:
a) Hyperpolarization
b) Depolarization
c) Sodium loss
d) Membrane stabilization only
Answer: b) Depolarization
- Depolarization opens which channels?
a) Chloride channels
b) Voltage-gated calcium channels
c) Sodium leak channels
d) Proton pumps
Answer: b) Voltage-gated calcium channels
- Increased intracellular calcium triggers:
a) Histamine release
b) Insulin exocytosis
c) Potassium efflux
d) ATP degradation
Answer: b) Insulin exocytosis
- Repaglinide is mainly used in:
a) Type 1 diabetes
b) Type 2 diabetes mellitus
c) Diabetes insipidus
d) Hyperthyroidism
Answer: b) Type 2 diabetes mellitus
- Repaglinide mainly controls:
a) Fasting hypoglycemia
b) Postprandial hyperglycemia
c) Ketoacidosis
d) Hypercalcemia
Answer: b) Postprandial hyperglycemia
- A common adverse effect is:
a) Hypoglycemia
b) Bradycardia
c) Hypernatremia
d) Severe hypotension
Answer: a) Hypoglycemia
- Repaglinide has which pharmacokinetic feature?
a) Slow onset and long duration
b) Rapid onset and short duration
c) No hepatic metabolism
d) Renal activation only
Answer: b) Rapid onset and short duration
- Repaglinide interacts with which receptor subunit?
a) SUR1
b) SUR2
c) β1 receptor
d) NMDA receptor
Answer: a) SUR1
- Compared with metformin, repaglinide primarily:
a) Improves insulin sensitivity only
b) Stimulates insulin secretion
c) Decreases glucose absorption only
d) Blocks glucagon release only
Answer: b) Stimulates insulin secretion
FAQs
What is the mechanism of action of repaglinide?
Repaglinide closes ATP-sensitive potassium channels in pancreatic β-cells, stimulating insulin secretion.
Why is repaglinide taken before meals?
Because it rapidly controls postprandial blood glucose levels.
What is the main adverse effect of repaglinide?
Hypoglycemia.
How does repaglinide differ from sulfonylureas?
It has a faster onset and shorter duration of action.
Can repaglinide be used in type 1 diabetes?
No, it requires functioning pancreatic β-cells.
Which enzyme systems metabolize repaglinide?
Mainly CYP3A4 and CYP2C8.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics – Antidiabetic Drugs
https://accessmedicine.mhmedical.com/book.aspx?bookid=3191
Katzung: Basic and Clinical Pharmacology – Drugs Used in Diabetes Mellitus
https://accessmedicine.mhmedical.com/content.aspx?bookid=3382
Tripathi: Essentials of Medical Pharmacology – Oral Antidiabetic Drugs
https://www.jaypeedigital.com
Harrison’s Principles of Internal Medicine – Diabetes Mellitus
https://accessmedicine.mhmedical.com

