Table of Contents
Introduction
Metoprolol is a selective β1-adrenergic receptor blocker (cardioselective beta-blocker) widely used in the management of hypertension, angina, heart failure, and arrhythmias. By selectively targeting β1 receptors in the heart, metoprolol reduces cardiac workload and oxygen demand while minimizing effects on β2 receptors in the lungs at therapeutic doses.
Mechanism of Action (Step-wise)
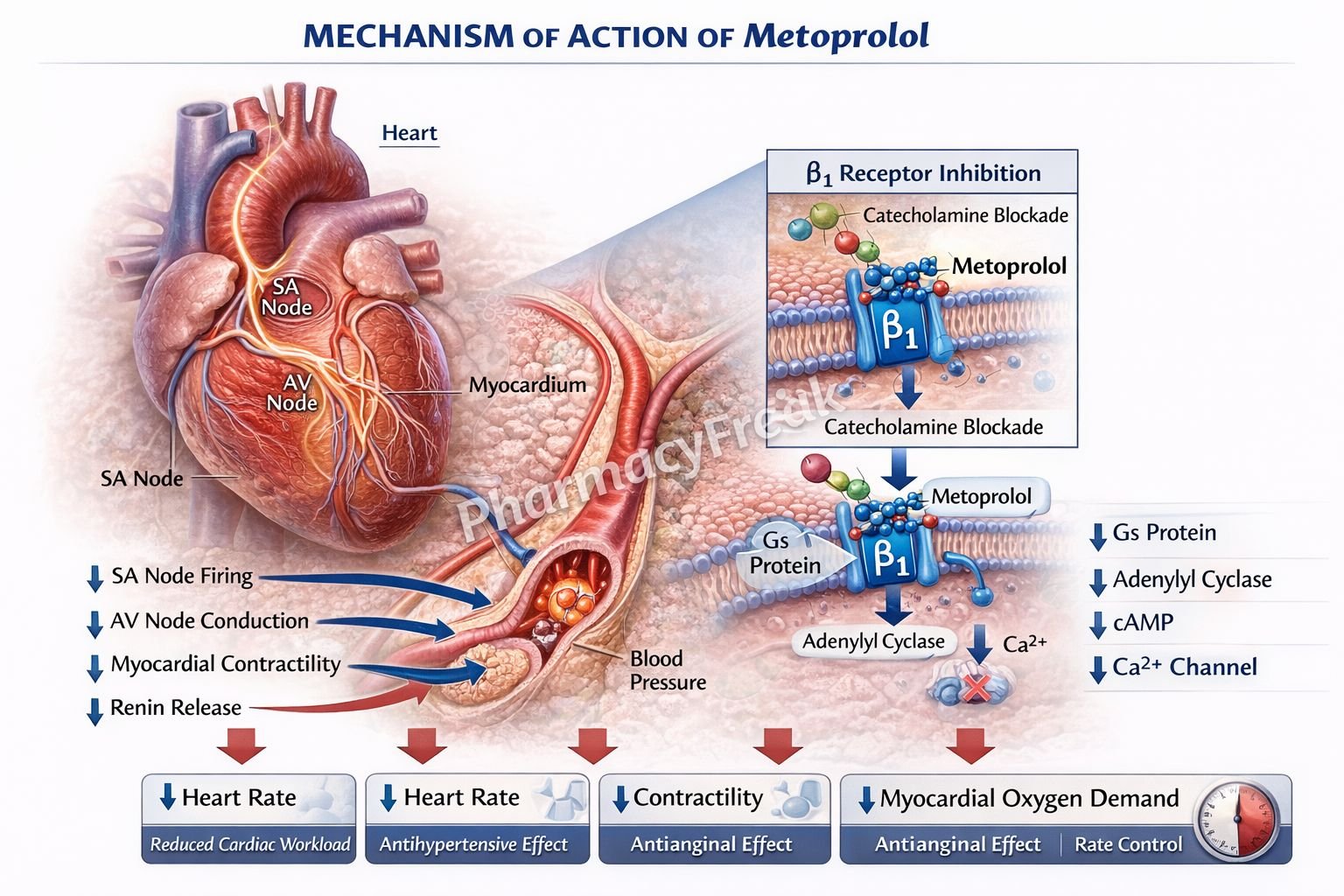
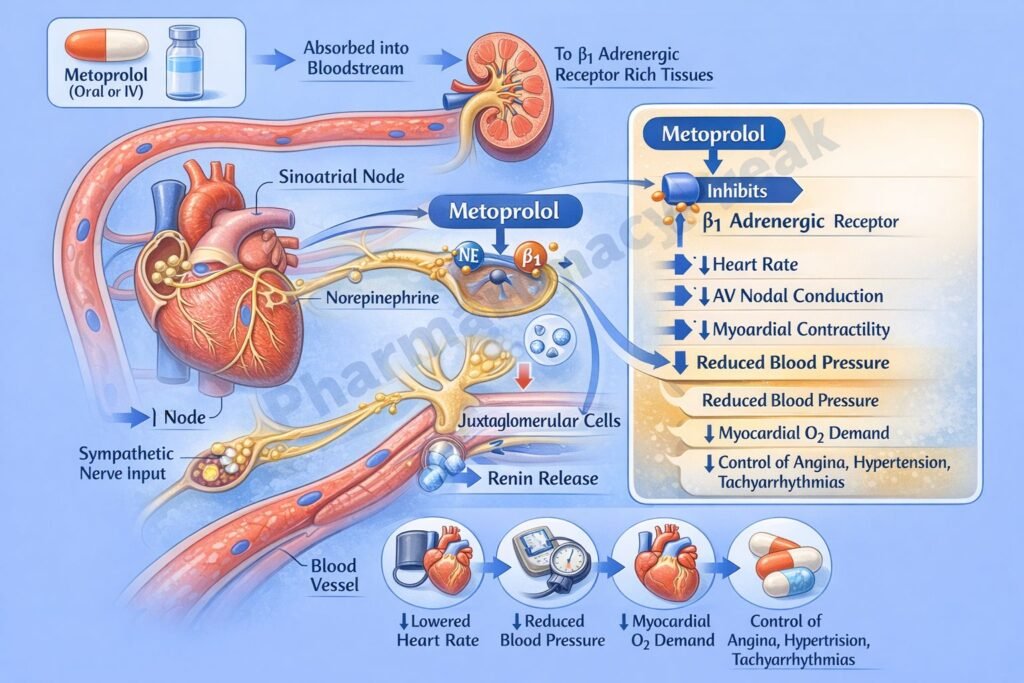
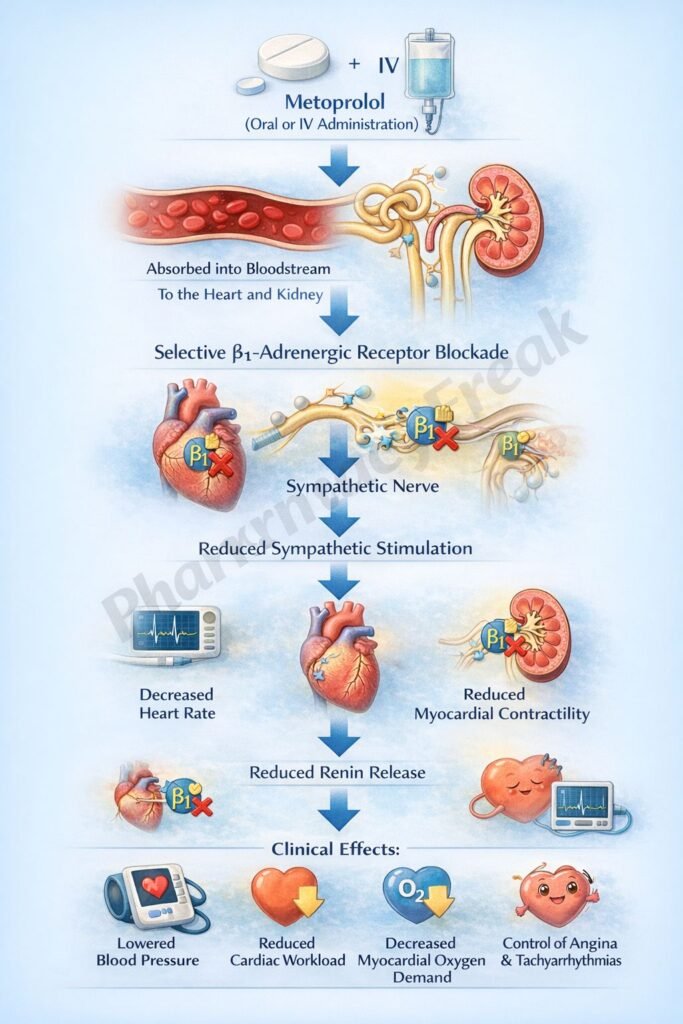
- Metoprolol selectively blocks β1-adrenergic receptors in the heart.
- These receptors are normally stimulated by catecholamines such as epinephrine and norepinephrine.
- Blocking β1 receptors decreases activation of adenylate cyclase.
- This reduces cyclic AMP (cAMP) levels in cardiac cells.
- Lower cAMP decreases calcium influx through voltage-gated calcium channels.
- Reduced intracellular calcium leads to decreased myocardial contractility (negative inotropic effect).
- It also reduces heart rate (negative chronotropic effect) by acting on the sinoatrial (SA) node.
- Conduction through the atrioventricular (AV) node is slowed (negative dromotropic effect).
- In the kidneys, β1 blockade reduces renin release from juxtaglomerular cells.
- This suppresses the renin-angiotensin-aldosterone system (RAAS), lowering blood pressure.
- The overall effect is decreased cardiac output and reduced blood pressure.
A key exam point is that metoprolol is a selective β1 blocker that reduces heart rate, contractility, and renin release.
Pharmacokinetics
Metoprolol is administered orally or intravenously. It undergoes extensive first-pass metabolism in the liver, resulting in moderate bioavailability. It is lipophilic and can cross the blood-brain barrier. It is metabolized primarily by CYP2D6 enzymes and excreted in urine. It has a relatively short half-life but is available in extended-release formulations for once-daily dosing.
Clinical Uses
Metoprolol is used in hypertension to reduce blood pressure and cardiovascular risk. It is also used in angina to decrease myocardial oxygen demand. In heart failure, it improves survival by reducing sympathetic overactivity. It is effective in controlling arrhythmias by slowing heart rate and AV conduction. Additionally, it is used in post-myocardial infarction patients to reduce mortality.
Adverse Effects
Common adverse effects include bradycardia, hypotension, fatigue, and dizziness. Because it is cardioselective, bronchoconstriction is less likely but can still occur at higher doses. It may cause worsening of heart failure in acute settings if not properly titrated. Other effects include depression, sexual dysfunction, and masking of hypoglycemia symptoms in diabetic patients.
Comparative Analysis
| Feature | Metoprolol | Propranolol | Atenolol |
|---|---|---|---|
| Selectivity | β1 selective | Non-selective (β1 + β2) | β1 selective |
| Lipophilicity | High | High | Low |
| CNS penetration | Yes | Yes | Minimal |
| Effect on lungs | Minimal (at low dose) | Significant | Minimal |
| Use in asthma | Caution | Contraindicated | Safer |
| Half-life | Moderate | Short | Longer |
Metoprolol differs from propranolol in being β1 selective, resulting in fewer respiratory side effects. Compared to atenolol, metoprolol is more lipophilic and crosses the blood-brain barrier, leading to more CNS effects.
MCQs
- Metoprolol primarily blocks which receptor?
a) α1 receptor
b) β1 receptor
c) β2 receptor
d) Dopamine receptor
Answer: b) β1 receptor
- β1 receptor blockade leads to decreased:
a) cAMP
b) Sodium
c) Potassium
d) Chloride
Answer: a) cAMP
- Reduced cAMP leads to decreased:
a) Calcium influx
b) Sodium influx
c) Potassium efflux
d) Chloride influx
Answer: a) Calcium influx
- Metoprolol decreases heart rate by acting on:
a) AV node only
b) SA node
c) Purkinje fibers
d) Ventricles only
Answer: b) SA node
- Metoprolol reduces contractility by:
a) Increasing calcium
b) Decreasing calcium
c) Increasing sodium
d) Blocking potassium
Answer: b) Decreasing calcium
- Metoprolol reduces renin release from:
a) Liver
b) Kidney
c) Brain
d) Heart
Answer: b) Kidney
- Metoprolol is used in:
a) Asthma
b) Hypertension
c) Diabetes
d) Anemia
Answer: b) Hypertension
- A common adverse effect is:
a) Tachycardia
b) Bradycardia
c) Hypercalcemia
d) Hyperglycemia
Answer: b) Bradycardia
- Compared to propranolol, metoprolol is:
a) Non-selective
b) β1 selective
c) β2 selective
d) Alpha blocker
Answer: b) β1 selective
- Metoprolol is metabolized mainly in the:
a) Kidney
b) Liver
c) Lung
d) Brain
Answer: b) Liver
- Metoprolol may mask symptoms of:
a) Hyperthyroidism
b) Hypoglycemia
c) Hypercalcemia
d) Hypertension
Answer: b) Hypoglycemia
- Metoprolol reduces blood pressure by:
a) Increasing cardiac output
b) Decreasing cardiac output
c) Increasing sodium retention
d) Increasing heart rate
Answer: b) Decreasing cardiac output
FAQs
What is the mechanism of action of metoprolol?
It selectively blocks β1 receptors, reducing heart rate, contractility, and renin release.
Why is metoprolol considered cardioselective?
Because it primarily blocks β1 receptors in the heart.
Does metoprolol affect the lungs?
At therapeutic doses, it has minimal effect on β2 receptors, but caution is still required in asthma.
What is the role of metoprolol in heart failure?
It reduces sympathetic overactivity and improves survival.
Why can metoprolol mask hypoglycemia?
It blocks sympathetic symptoms like tachycardia.
Can metoprolol cross the blood-brain barrier?
Yes, due to its lipophilicity.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics – Adrenergic Drugs
https://accessmedicine.mhmedical.com/book.aspx?bookid=3191
Katzung: Basic and Clinical Pharmacology – Beta Blockers
https://accessmedicine.mhmedical.com/content.aspx?bookid=3382
Tripathi: Essentials of Medical Pharmacology – Adrenergic Drugs
https://www.jaypeedigital.com
Harrison’s Principles of Internal Medicine – Cardiovascular Pharmacology
https://accessmedicine.mhmedical.com


