Table of Contents
Introduction
Metoclopramide is a prokinetic and antiemetic drug commonly used in gastrointestinal disorders and nausea-related conditions. It enhances gastrointestinal motility and accelerates gastric emptying while also acting centrally to reduce nausea and vomiting. It is widely used in conditions such as gastroparesis, gastroesophageal reflux disease (GERD), and chemotherapy-induced nausea.
Mechanism of Action (Step-wise)
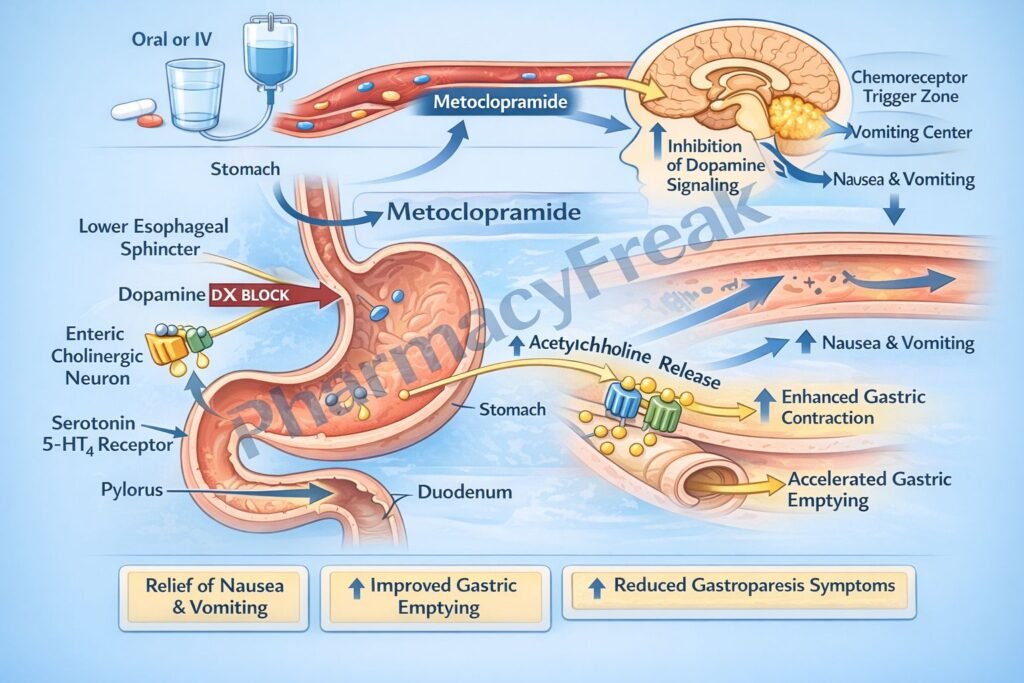
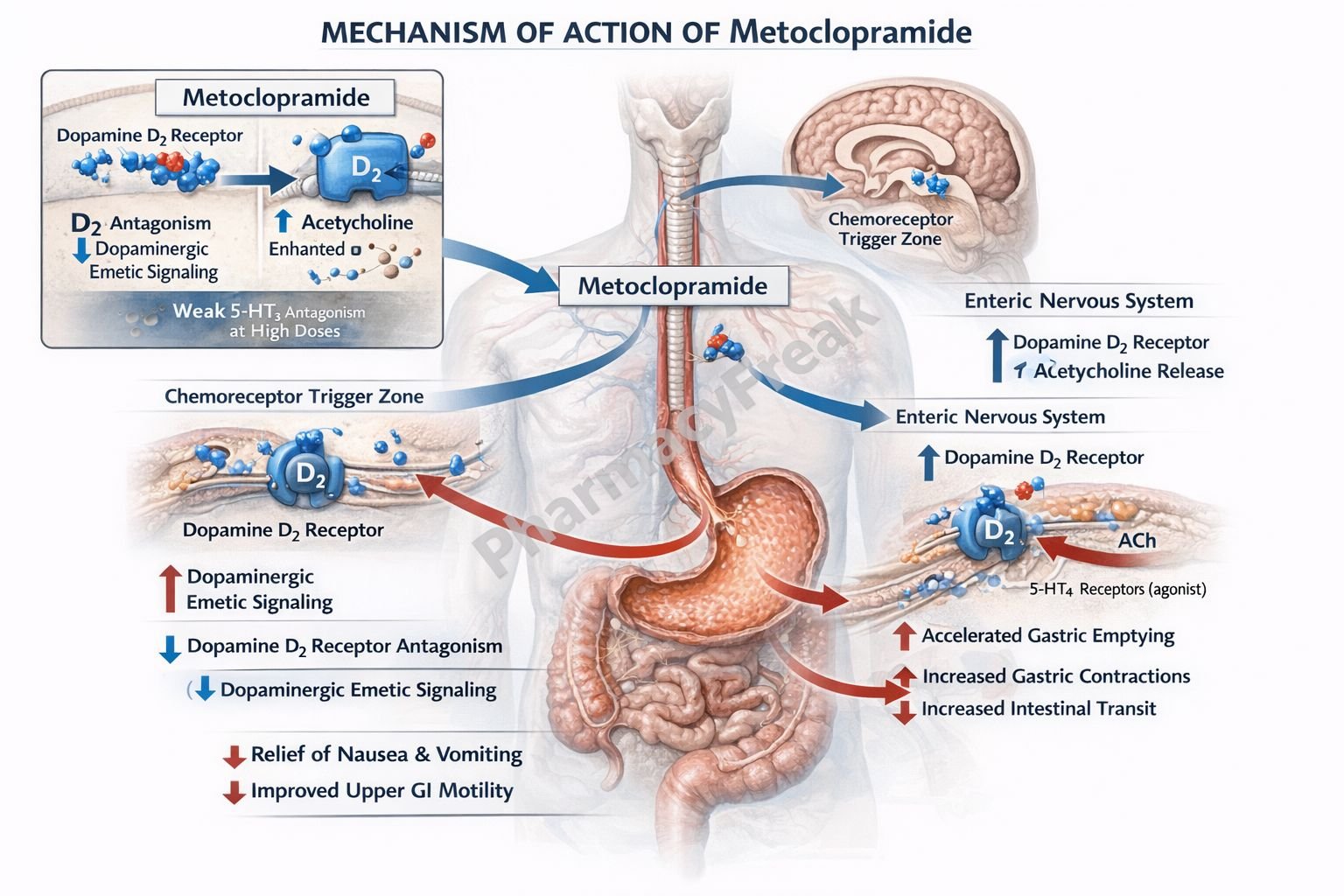
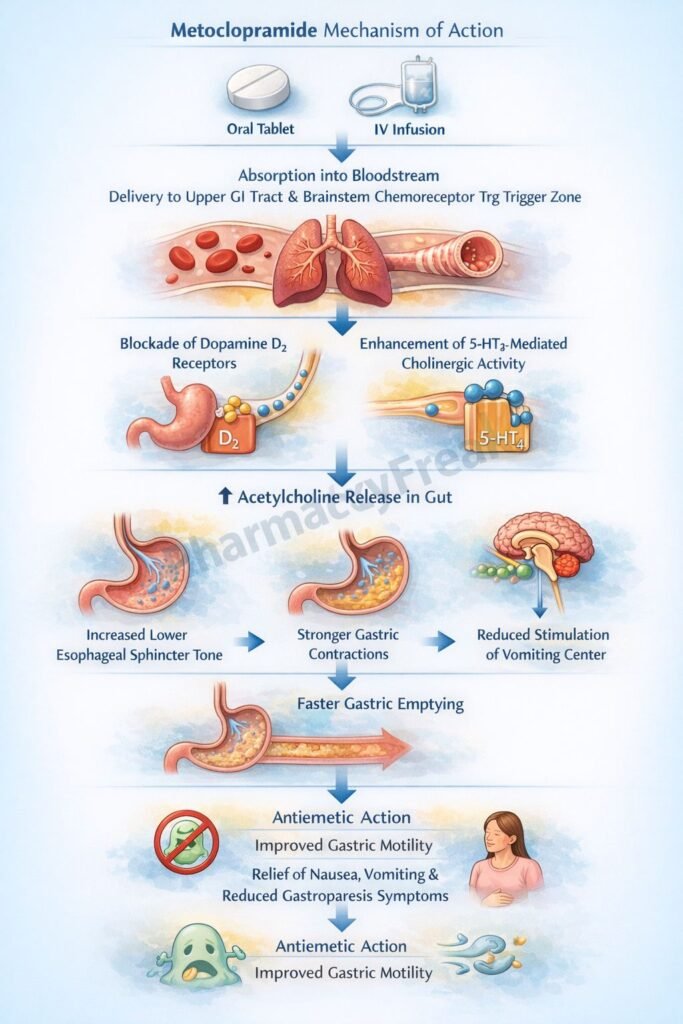
- Metoclopramide acts as an antagonist at dopamine D2 receptors.
- In the chemoreceptor trigger zone (CTZ), D2 receptor blockade reduces nausea and vomiting.
- In the gastrointestinal tract, D2 receptor blockade enhances cholinergic activity.
- This increases acetylcholine release in the enteric nervous system.
- Increased acetylcholine stimulates smooth muscle contraction.
- This enhances gastric emptying and increases intestinal motility.
- Metoclopramide also acts as a 5-HT4 receptor agonist.
- Activation of 5-HT4 receptors further increases acetylcholine release.
- At higher doses, it may block 5-HT3 receptors, contributing to antiemetic effects.
- It increases lower esophageal sphincter (LES) tone.
- The combined effects improve gastric motility and reduce reflux and nausea.
A key exam point is that metoclopramide is a D2 antagonist with 5-HT4 agonist activity that enhances GI motility and acts as an antiemetic.
Pharmacokinetics
Metoclopramide is administered orally, intravenously, or intramuscularly. It is well absorbed and has moderate bioavailability. It crosses the blood-brain barrier, which explains its central effects and adverse reactions. It is metabolized in the liver and excreted primarily via the kidneys. Dose adjustment is required in renal impairment. It has a relatively short half-life, requiring multiple daily dosing.
Clinical Uses
Metoclopramide is used in gastroparesis, especially in diabetic patients, to improve gastric emptying. It is also used in gastroesophageal reflux disease to increase lower esophageal sphincter tone. As an antiemetic, it is used in chemotherapy-induced nausea, postoperative nausea, and vomiting. It is also used in migraine to enhance absorption of oral medications.
Adverse Effects
Common adverse effects include drowsiness, fatigue, and restlessness. Because it blocks dopamine receptors in the CNS, it can cause extrapyramidal symptoms such as dystonia, akathisia, and parkinsonism. Long-term use may lead to tardive dyskinesia, a serious and potentially irreversible condition. Hyperprolactinemia may occur due to dopamine blockade. These effects are important exam points.
Comparative Analysis
| Feature | Metoclopramide | Domperidone | Ondansetron |
|---|---|---|---|
| Mechanism | D2 antagonist + 5-HT4 agonist | Peripheral D2 antagonist | 5-HT3 antagonist |
| CNS penetration | High | Low | Moderate |
| Prokinetic effect | Strong | Moderate | None |
| Antiemetic action | Yes | Yes | Yes |
| EPS risk | High | Low | None |
| Use | Gastroparesis, nausea | Nausea, GI disorders | Chemotherapy-induced nausea |
Metoclopramide differs from domperidone in that it crosses the blood-brain barrier and has higher risk of extrapyramidal side effects. Compared to ondansetron, it has prokinetic effects but less selective antiemetic action.
MCQs
- Metoclopramide primarily blocks which receptor?
a) H1 receptor
b) D2 receptor
c) Beta receptor
d) Alpha receptor
Answer: b) D2 receptor
- Metoclopramide acts in the CTZ to:
a) Increase vomiting
b) Reduce vomiting
c) Increase acid
d) Reduce motility
Answer: b) Reduce vomiting
- Metoclopramide increases GI motility by:
a) Decreasing acetylcholine
b) Increasing acetylcholine
c) Blocking sodium
d) Blocking calcium
Answer: b) Increasing acetylcholine
- Metoclopramide is also a:
a) 5-HT3 agonist
b) 5-HT4 agonist
c) H2 blocker
d) Alpha blocker
Answer: b) 5-HT4 agonist
- It increases tone of:
a) Pyloric sphincter
b) Lower esophageal sphincter
c) Anal sphincter
d) Bladder
Answer: b) Lower esophageal sphincter
- Metoclopramide is used in:
a) Hypertension
b) Gastroparesis
c) Diabetes only
d) Asthma
Answer: b) Gastroparesis
- A major adverse effect is:
a) Hypoglycemia
b) Extrapyramidal symptoms
c) Hypercalcemia
d) Bradycardia
Answer: b) Extrapyramidal symptoms
- Long-term use may cause:
a) Hypertension
b) Tardive dyskinesia
c) Hypokalemia
d) Arrhythmia
Answer: b) Tardive dyskinesia
- Metoclopramide increases prolactin by:
a) Increasing dopamine
b) Blocking dopamine
c) Increasing serotonin
d) Blocking histamine
Answer: b) Blocking dopamine
- Compared to domperidone, metoclopramide:
a) Does not cross BBB
b) Crosses BBB
c) Has no CNS effects
d) Is less effective
Answer: b) Crosses BBB
- Metoclopramide is metabolized in the:
a) Kidney
b) Liver
c) Lung
d) Brain
Answer: b) Liver
- Metoclopramide enhances gastric emptying by:
a) Relaxing smooth muscle
b) Increasing peristalsis
c) Blocking acid
d) Decreasing enzymes
Answer: b) Increasing peristalsis
FAQs
What is the mechanism of action of metoclopramide?
It blocks D2 receptors and stimulates 5-HT4 receptors, increasing GI motility and reducing nausea.
Why does metoclopramide cause extrapyramidal symptoms?
Because it blocks dopamine receptors in the central nervous system.
What is its role in gastroparesis?
It enhances gastric emptying by increasing motility.
Does metoclopramide cross the blood-brain barrier?
Yes, which explains its CNS effects.
What is a serious long-term adverse effect?
Tardive dyskinesia.
How does it help in GERD?
By increasing lower esophageal sphincter tone.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics – GI Drugs
https://accessmedicine.mhmedical.com/book.aspx?bookid=3191
Katzung: Basic and Clinical Pharmacology – Antiemetics
https://accessmedicine.mhmedical.com/content.aspx?bookid=3382
Tripathi: Essentials of Medical Pharmacology – GI Pharmacology
https://www.jaypeedigital.com
Harrison’s Principles of Internal Medicine – Gastrointestinal Disorders
https://accessmedicine.mhmedical.com