Table of Contents
Introduction
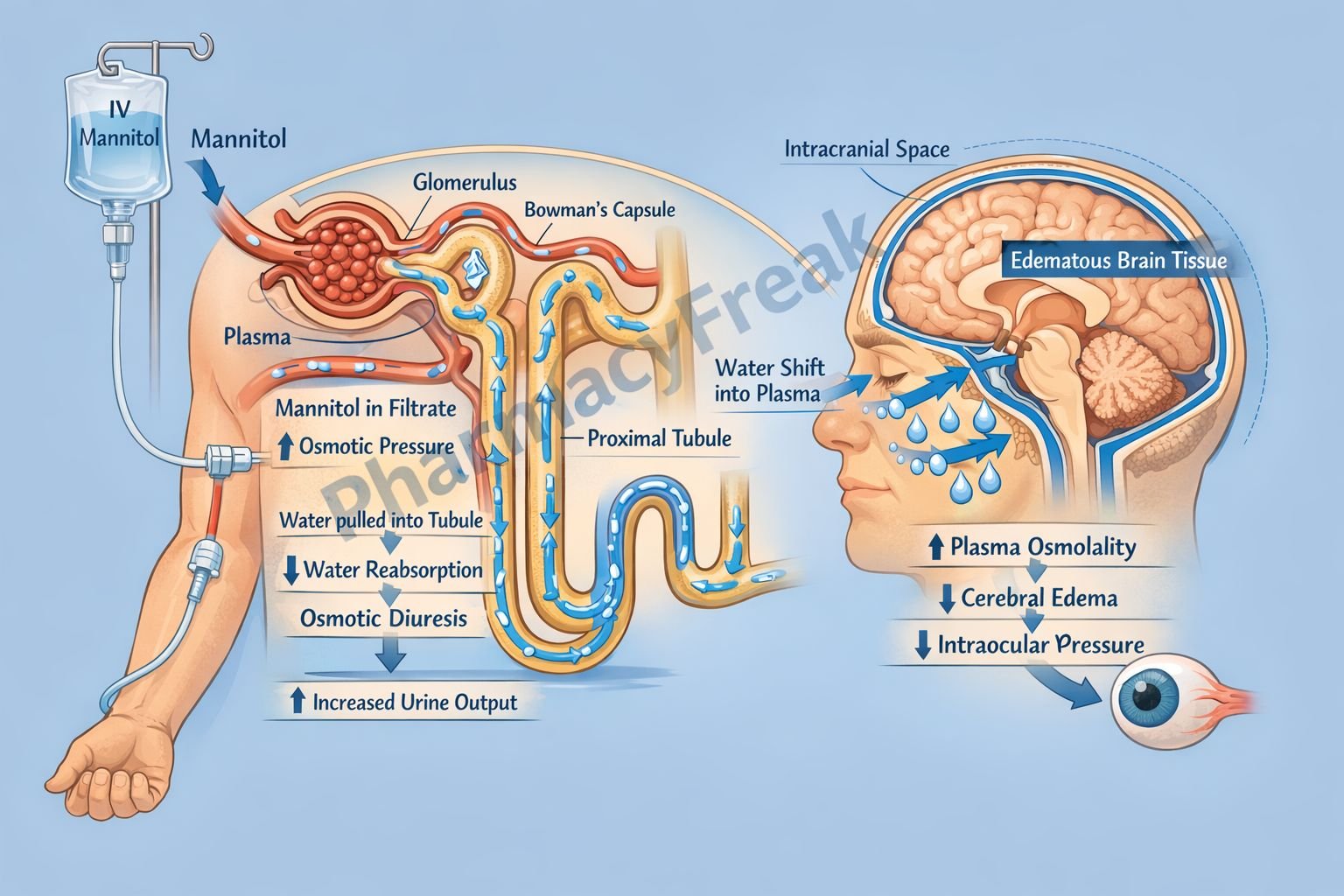
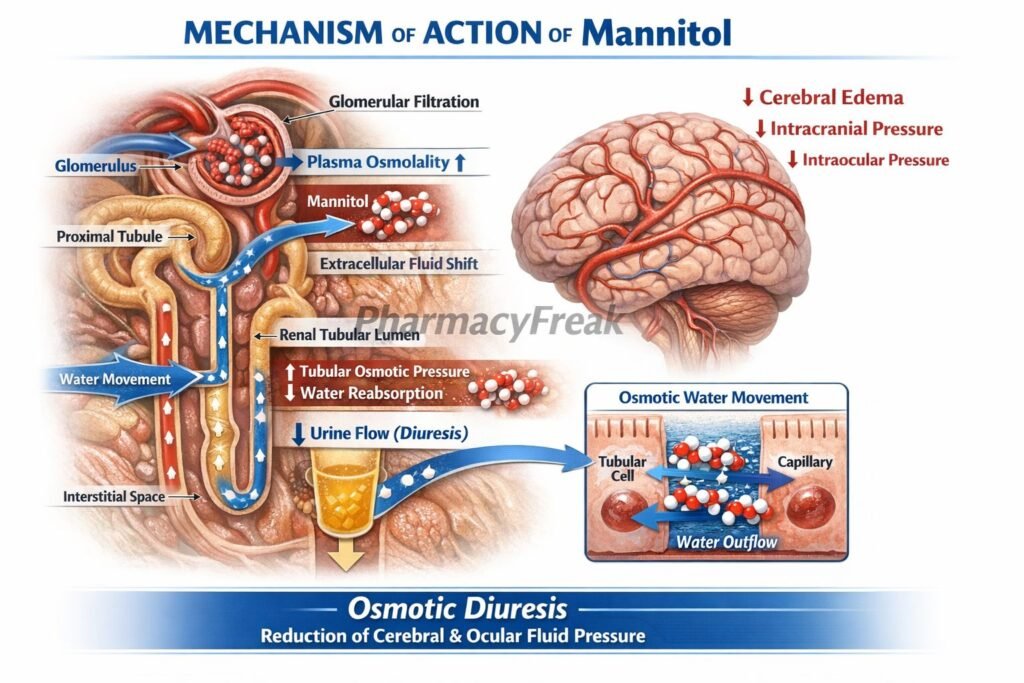
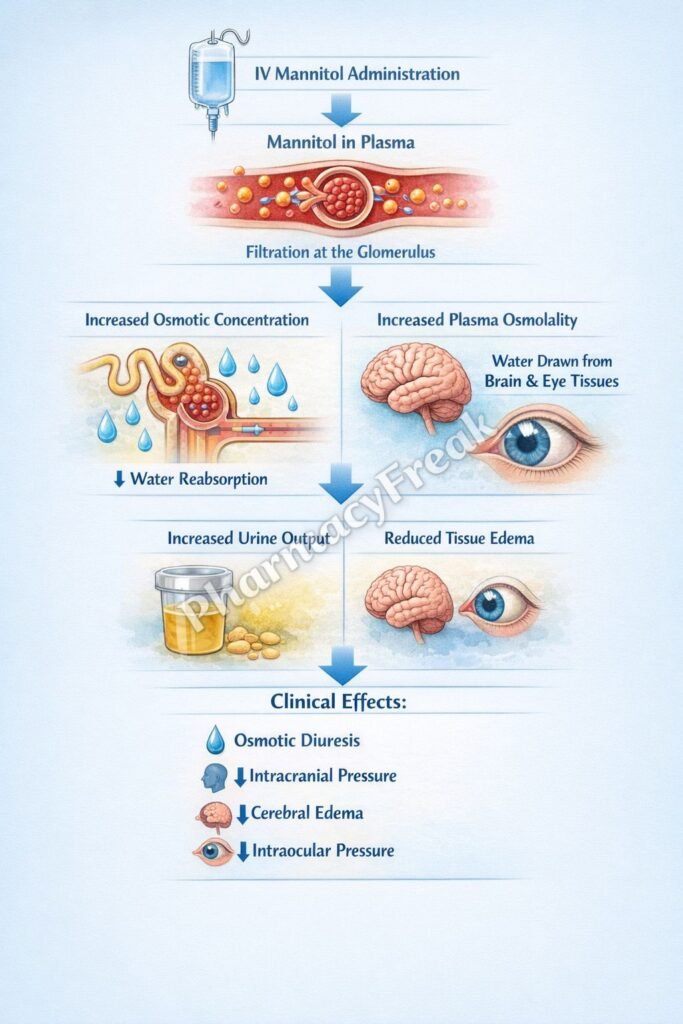
Mannitol is an osmotic diuretic widely used in clinical practice to reduce intracranial pressure, intraocular pressure, and to promote diuresis in certain renal conditions. It is a pharmacologically inert sugar alcohol that is freely filtered at the glomerulus but not reabsorbed in the renal tubules. Its primary mechanism involves increasing osmotic pressure in the tubular fluid, thereby preventing water reabsorption.
Mechanism of Action (Step-wise)
- Mannitol is administered intravenously and freely filtered by the glomerulus.
- It is not reabsorbed in the renal tubules.
- It increases osmotic pressure in the tubular lumen.
- This reduces passive water reabsorption in the proximal tubule and descending limb of the loop of Henle.
- Increased tubular fluid volume leads to enhanced urine output (diuresis).
- Mannitol also decreases sodium reabsorption by diluting tubular fluid.
- In the brain, it increases plasma osmolarity, drawing water out of cerebral tissues into the intravascular space.
- This reduces intracranial pressure and cerebral edema.
- Similarly, it reduces intraocular pressure by shifting fluid from the eye into circulation.
A key exam point is that mannitol acts by osmotic diuresis and fluid shift from tissues to plasma.
Pharmacokinetics
Mannitol is administered intravenously because it is poorly absorbed orally for systemic effects. It is not metabolized and remains largely confined to the extracellular compartment. It is eliminated unchanged by the kidneys via glomerular filtration. Its onset of action is rapid, especially in reducing intracranial pressure. The duration of action depends on renal function. In renal impairment, accumulation can occur, leading to adverse effects.
Clinical Uses
Mannitol is used to reduce intracranial pressure in conditions such as cerebral edema, head injury, and intracranial hemorrhage. It is also used to reduce intraocular pressure in acute glaucoma. In addition, it is used to promote diuresis in acute renal failure and to prevent renal damage in situations such as rhabdomyolysis. It may also be used to enhance elimination of certain toxins.
Adverse Effects
Adverse effects of mannitol include dehydration, electrolyte imbalance, and hypotension. Initially, it can cause expansion of extracellular fluid volume, which may lead to pulmonary edema, especially in patients with heart failure. Headache, nausea, and vomiting may also occur. In severe cases, excessive use can lead to hyperosmolarity and renal impairment.
Comparative Analysis
| Feature | Mannitol | Loop Diuretics | Thiazide Diuretics |
|---|---|---|---|
| Class | Osmotic diuretic | High-ceiling diuretic | Moderate diuretic |
| Site of action | Proximal tubule & descending limb | Thick ascending limb | Distal convoluted tubule |
| Mechanism | Osmotic effect | NKCC2 inhibition | Na⁺/Cl⁻ inhibition |
| Effect on ICP | Decreases | No direct effect | No direct effect |
| Route | IV | Oral/IV | Oral |
| Major use | Cerebral edema | Edema, CHF | Hypertension |
Mannitol differs from other diuretics because it does not act on specific transporters but instead increases osmotic pressure to draw water into the tubular lumen. It is uniquely useful in reducing intracranial and intraocular pressure.
MCQs
- Mannitol belongs to which class of diuretics?
a) Loop diuretics
b) Thiazide diuretics
c) Osmotic diuretics
d) Potassium-sparing diuretics
Answer: c) Osmotic diuretics
- Mannitol is primarily administered via:
a) Oral route
b) Intravenous route
c) Intramuscular route
d) Subcutaneous route
Answer: b) Intravenous route
- Mannitol increases osmotic pressure in:
a) Blood only
b) Tubular lumen
c) Liver cells
d) Brain cells
Answer: b) Tubular lumen
- Mannitol reduces water reabsorption in:
a) Collecting duct only
b) Proximal tubule and descending limb
c) Distal tubule only
d) Glomerulus
Answer: b) Proximal tubule and descending limb
- Mannitol is not reabsorbed in the:
a) Glomerulus
b) Renal tubules
c) Liver
d) Intestine
Answer: b) Renal tubules
- Mannitol is mainly used to reduce:
a) Blood glucose
b) Intracranial pressure
c) Heart rate
d) Thyroid hormones
Answer: b) Intracranial pressure
- Mannitol draws water from:
a) Blood to tissues
b) Tissues to blood
c) Kidney to liver
d) Lungs to heart
Answer: b) Tissues to blood
- Mannitol is eliminated via:
a) Liver metabolism
b) Kidney unchanged
c) Lungs
d) Skin
Answer: b) Kidney unchanged
- A major adverse effect is:
a) Hypoglycemia
b) Pulmonary edema
c) Bradycardia
d) Hypercalcemia
Answer: b) Pulmonary edema
- Mannitol initially causes:
a) Dehydration only
b) Volume expansion
c) Hypotension only
d) Hyperkalemia
Answer: b) Volume expansion
- Mannitol is useful in:
a) Asthma
b) Acute glaucoma
c) Diabetes mellitus
d) Hypertension only
Answer: b) Acute glaucoma
- Mannitol acts by:
a) Blocking sodium channels
b) Osmotic effect
c) Increasing aldosterone
d) Blocking calcium channels
Answer: b) Osmotic effect
FAQs
What is the mechanism of action of mannitol?
Mannitol increases osmotic pressure in renal tubules, reducing water reabsorption and causing diuresis.
Why is mannitol used in cerebral edema?
It increases plasma osmolarity and draws water out of brain tissue.
Does mannitol undergo metabolism?
No, it is excreted unchanged by the kidneys.
Why is mannitol given intravenously?
It is poorly absorbed orally for systemic diuretic effect.
What is a major risk of mannitol therapy?
Pulmonary edema due to fluid shifts.
Can mannitol be used in renal failure?
Use cautiously; accumulation can occur if renal function is impaired.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics – Diuretics
https://accessmedicine.mhmedical.com/book.aspx?bookid=3191
Katzung: Basic and Clinical Pharmacology – Diuretics
https://accessmedicine.mhmedical.com/content.aspx?bookid=3382
Tripathi: Essentials of Medical Pharmacology – Diuretics
https://www.jaypeedigital.com
Harrison’s Principles of Internal Medicine – Fluid and Electrolyte Disorders
https://accessmedicine.mhmedical.com


