Table of Contents
Introduction
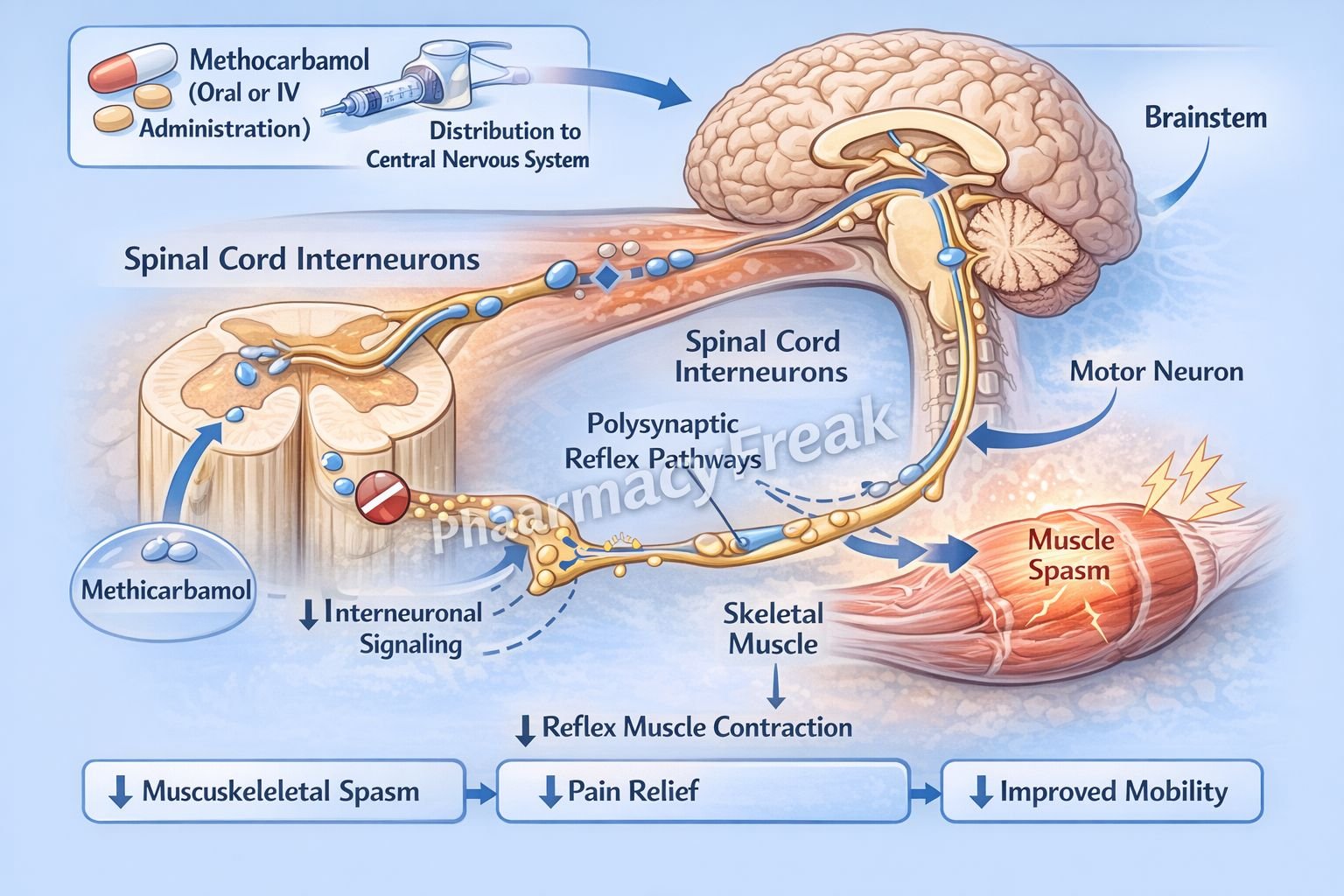
Methocarbamol is a centrally acting muscle relaxant used in the management of acute musculoskeletal pain and muscle spasms. It is commonly prescribed in conditions such as back pain, muscle strain, and injury-related spasms. Unlike neuromuscular blockers, methocarbamol does not act directly on skeletal muscle or the neuromuscular junction. Instead, it exerts its effect within the central nervous system to reduce muscle hyperactivity.
Mechanism of Action (Step-wise)
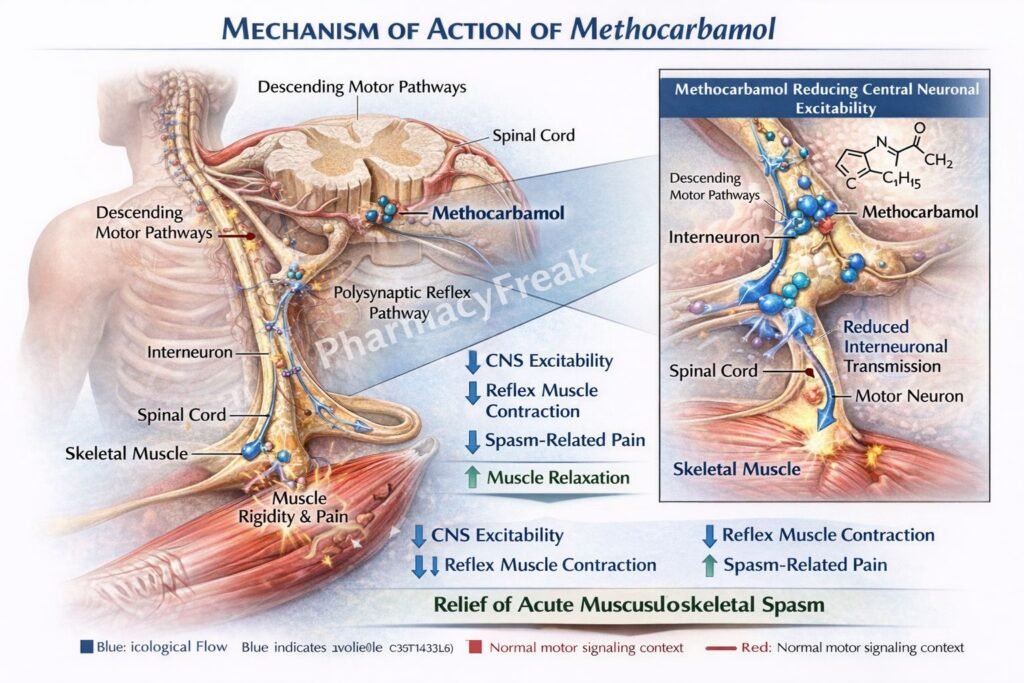
- Methocarbamol acts centrally in the brain and spinal cord.
- It produces general CNS depression rather than a specific receptor-mediated action.
- It reduces polysynaptic reflex activity in the spinal cord.
- This decreases transmission of nerve impulses responsible for muscle spasms.
- It leads to reduced muscle tone and relief of muscle spasm.
- The exact molecular mechanism is not fully understood.
- It does not directly affect skeletal muscle contraction or neuromuscular transmission.
- The net effect is muscle relaxation and pain relief due to decreased reflex activity.
A key exam point is that methocarbamol is a centrally acting muscle relaxant with an unclear exact mechanism but reduces polysynaptic reflexes.

Pharmacokinetics
Methocarbamol is administered orally or intravenously. It is rapidly absorbed after oral administration and has a relatively short onset of action. It is metabolized in the liver via dealkylation and hydroxylation. The metabolites and a small amount of unchanged drug are excreted in urine. Its half-life is relatively short, requiring multiple daily dosing. It does not accumulate significantly with normal dosing.
Clinical Uses
Methocarbamol is used in the treatment of acute musculoskeletal conditions such as muscle spasms, sprains, and strains. It is often used as an adjunct to rest, physical therapy, and analgesics. It may also be used in conditions such as tetanus as supportive therapy. It helps reduce pain and improve mobility by relieving muscle spasm.
Adverse Effects
Common adverse effects include drowsiness, dizziness, lightheadedness, and sedation due to its CNS depressant action. Other effects may include nausea, blurred vision, and headache. High doses or rapid intravenous administration may cause hypotension or bradycardia. Patients should be cautioned about activities requiring alertness such as driving.
Comparative Analysis
| Feature | Methocarbamol | Baclofen | Diazepam |
|---|---|---|---|
| Class | Central muscle relaxant | GABA-B agonist | Benzodiazepine |
| Mechanism | CNS depression (unknown exact) | GABA-B receptor activation | GABA-A enhancement |
| Site of action | CNS | Spinal cord | CNS |
| Sedation | Moderate | Moderate | High |
| Use | Acute muscle spasm | Spasticity | Muscle spasm, anxiety |
| Dependence risk | Low | Low | Higher |
Methocarbamol differs from baclofen and diazepam in that its mechanism is less specific and primarily involves general CNS depression. Baclofen acts specifically on GABA-B receptors, while diazepam enhances GABA-A receptor activity and has a higher risk of dependence.
MCQs
- Methocarbamol belongs to which class?
a) Neuromuscular blocker
b) Central muscle relaxant
c) Antidepressant
d) Antipsychotic
Answer: b) Central muscle relaxant
- Methocarbamol acts primarily on:
a) Skeletal muscle
b) Neuromuscular junction
c) Central nervous system
d) Peripheral nerves
Answer: c) Central nervous system
- The exact mechanism of methocarbamol is:
a) Fully understood
b) Unknown
c) Sodium channel blockade
d) Calcium channel blockade
Answer: b) Unknown
- Methocarbamol reduces:
a) Monosynaptic reflexes
b) Polysynaptic reflexes
c) Hormone release
d) Blood pressure
Answer: b) Polysynaptic reflexes
- Methocarbamol does NOT act on:
a) CNS
b) Spinal cord
c) Skeletal muscle directly
d) Brain
Answer: c) Skeletal muscle directly
- Methocarbamol is used in:
a) Hypertension
b) Muscle spasms
c) Diabetes
d) Asthma
Answer: b) Muscle spasms
- A common adverse effect is:
a) Hyperglycemia
b) Sedation
c) Hypertension
d) Hypokalemia
Answer: b) Sedation
- Methocarbamol is metabolized in the:
a) Kidney
b) Liver
c) Lung
d) Brain
Answer: b) Liver
- Compared to diazepam, methocarbamol has:
a) Higher dependence risk
b) Lower dependence risk
c) Same dependence risk
d) No effect
Answer: b) Lower dependence risk
- Methocarbamol is given as adjunct therapy with:
a) Surgery only
b) Rest and physical therapy
c) Insulin
d) Antibiotics
Answer: b) Rest and physical therapy
- Methocarbamol reduces muscle spasm by:
a) Direct muscle relaxation
b) CNS depression
c) Blocking acetylcholine
d) Increasing calcium
Answer: b) CNS depression
- IV methocarbamol may cause:
a) Hyperglycemia
b) Hypotension
c) Hypercalcemia
d) Tachycardia
Answer: b) Hypotension
FAQs
What is the mechanism of action of methocarbamol?
It acts centrally to depress CNS activity and reduce polysynaptic reflexes, leading to muscle relaxation.
Does methocarbamol act directly on muscles?
No, it does not directly affect skeletal muscle or neuromuscular transmission.
What is the main use of methocarbamol?
Relief of acute musculoskeletal pain and muscle spasms.
Why does methocarbamol cause drowsiness?
Due to its CNS depressant effects.
Is methocarbamol addictive?
It has low dependence potential compared to benzodiazepines.
Can methocarbamol be given intravenously?
Yes, but rapid administration may cause hypotension.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics – Muscle Relaxants
https://accessmedicine.mhmedical.com/book.aspx?bookid=3191
Katzung: Basic and Clinical Pharmacology – Skeletal Muscle Relaxants
https://accessmedicine.mhmedical.com/content.aspx?bookid=3382
Tripathi: Essentials of Medical Pharmacology – Muscle Relaxants
https://www.jaypeedigital.com
Harrison’s Principles of Internal Medicine – Musculoskeletal Disorders
https://accessmedicine.mhmedical.com

