Table of Contents
Introduction
Methadone is a long-acting synthetic opioid used in the management of chronic pain and opioid dependence. It is particularly important in opioid substitution therapy due to its ability to reduce withdrawal symptoms and cravings. Methadone has unique pharmacological properties compared to other opioids, including additional effects on NMDA receptors, which contribute to its analgesic and anti-hyperalgesic actions.
Mechanism of Action (Step-wise)
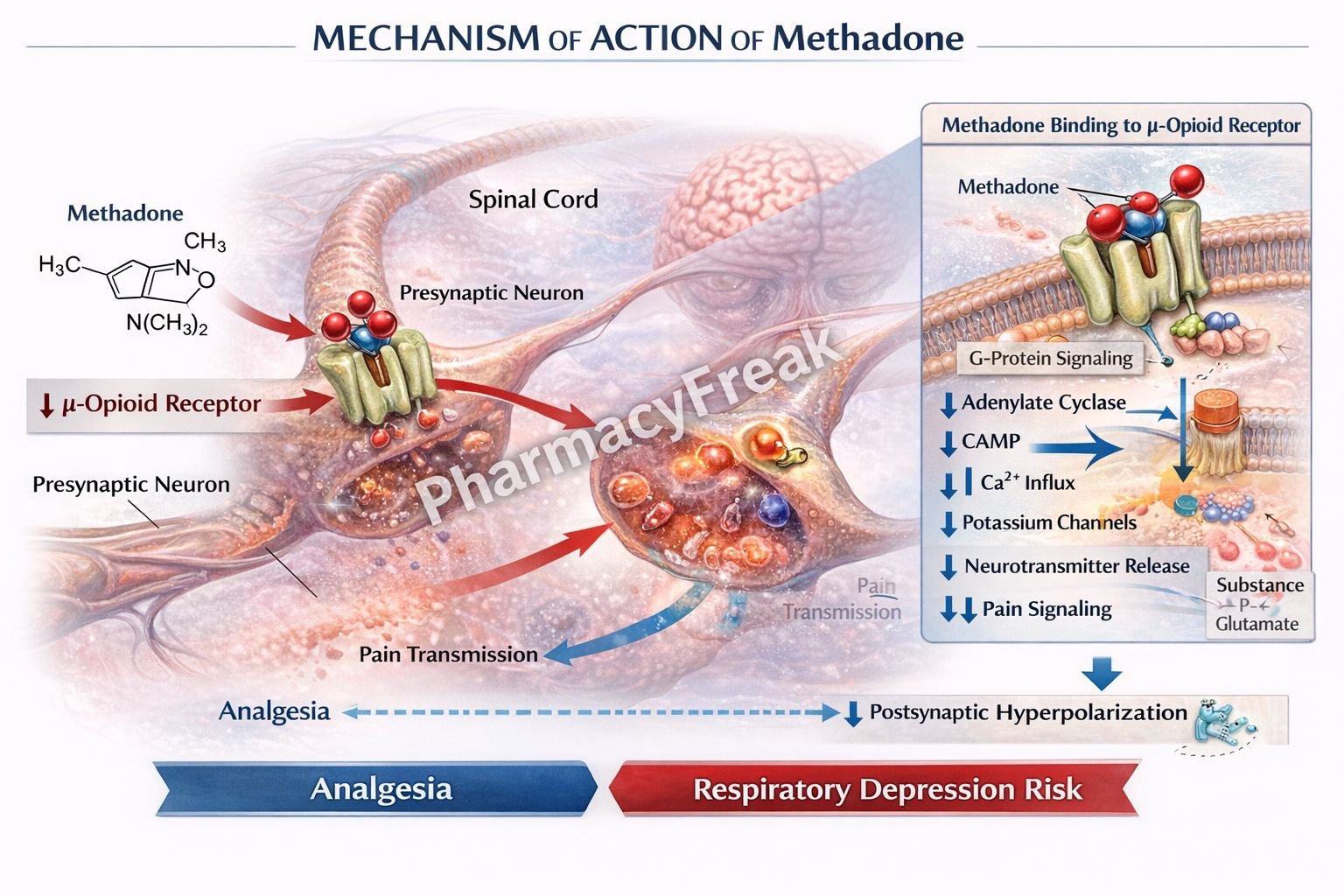
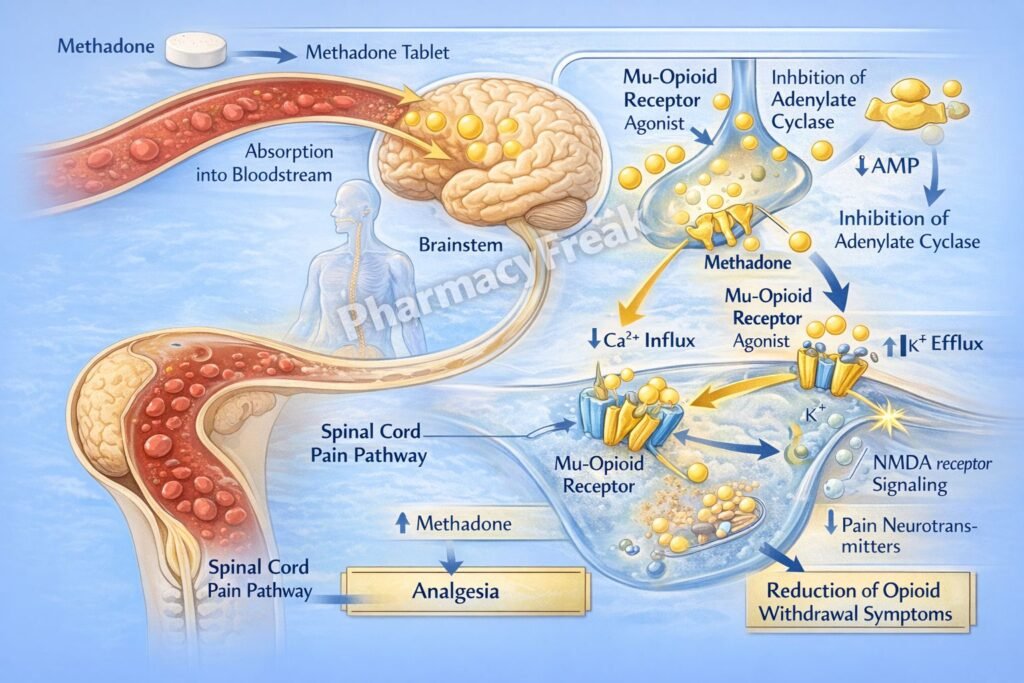
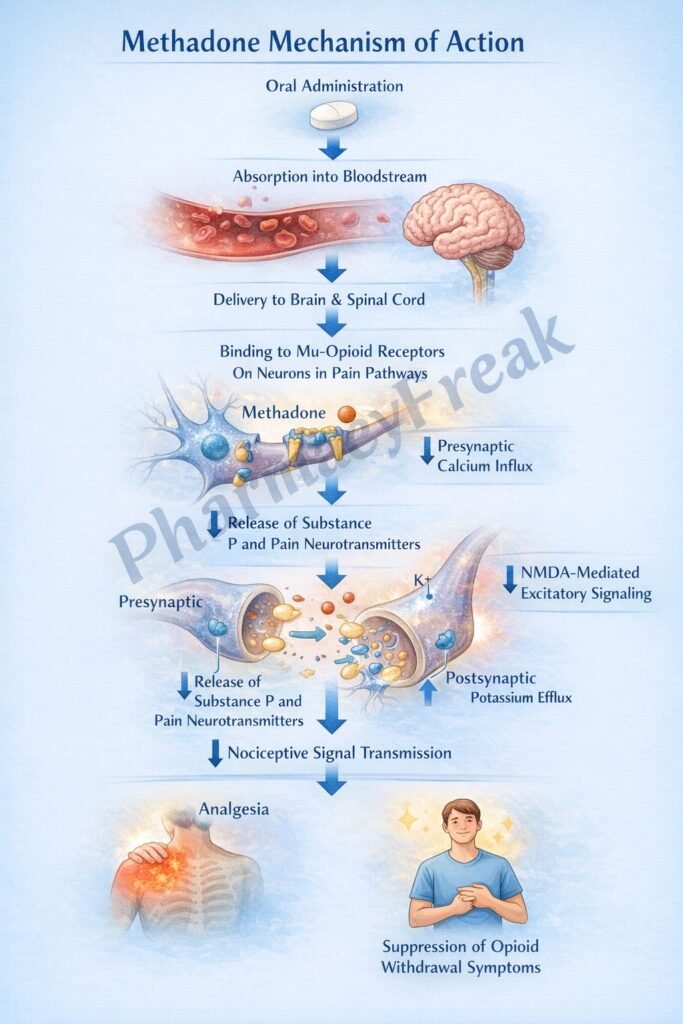
- Methadone acts as a full agonist at μ-opioid receptors in the central nervous system.
- Activation of μ-opioid receptors inhibits adenylate cyclase activity.
- This reduces cyclic AMP (cAMP) levels inside neurons.
- Methadone promotes opening of potassium channels, causing potassium efflux.
- This leads to hyperpolarization of neurons.
- It also inhibits voltage-gated calcium channels, reducing calcium influx.
- Reduced calcium entry decreases release of excitatory neurotransmitters such as glutamate and substance P.
- These effects result in decreased neuronal excitability and analgesia.
- Methadone also antagonizes NMDA (N-methyl-D-aspartate) receptors.
- NMDA receptor blockade reduces central sensitization and neuropathic pain.
- The combined opioid agonism and NMDA antagonism enhance its effectiveness in chronic and opioid-resistant pain.
A key exam point is that methadone is a μ-opioid receptor agonist with additional NMDA receptor antagonism.
Pharmacokinetics
Methadone is well absorbed orally and has high bioavailability. It has a long and variable half-life (ranging from about 8 to over 50 hours), which allows once-daily dosing in opioid dependence therapy. It is highly protein-bound and extensively metabolized in the liver via cytochrome P450 enzymes. Methadone is excreted in urine and feces. Its long half-life increases the risk of accumulation and requires careful dose titration.
Clinical Uses
Methadone is used in opioid dependence as maintenance therapy to prevent withdrawal and reduce cravings. It is also used in chronic pain management, particularly for severe or neuropathic pain. Its long duration of action makes it suitable for sustained analgesia. It is also useful in patients who require long-term opioid therapy with stable plasma levels.
Adverse Effects
Methadone shares common opioid-related adverse effects such as respiratory depression, sedation, constipation, nausea, and miosis. A unique and important adverse effect is QT interval prolongation, which can lead to torsades de pointes. Because of its long half-life, there is a risk of drug accumulation and delayed toxicity. Dependence and withdrawal symptoms may occur with long-term use. Caution is required when combined with other CNS depressants.
Comparative Analysis
| Feature | Methadone | Morphine | Buprenorphine |
|---|---|---|---|
| Receptor activity | Full μ agonist + NMDA antagonist | Full μ agonist | Partial μ agonist |
| Duration | Long | Short | Long |
| Use in dependence | Yes | No | Yes |
| NMDA effect | Present | Absent | Minimal |
| Risk of QT prolongation | Yes | No | Rare |
| Withdrawal suppression | Strong | Moderate | Moderate |
Methadone differs from morphine by having a longer duration of action and NMDA receptor antagonism. Compared to buprenorphine, methadone is a full agonist, producing stronger opioid effects and more effective suppression of withdrawal symptoms.
MCQs
- Methadone acts primarily on which receptor?
a) Dopamine receptor
b) μ-opioid receptor
c) Serotonin receptor
d) Histamine receptor
Answer: b) μ-opioid receptor
- Methadone also blocks which receptor?
a) GABA-A
b) NMDA
c) Dopamine D2
d) Alpha receptor
Answer: b) NMDA
- Methadone reduces cAMP by:
a) Activating adenylate cyclase
b) Inhibiting adenylate cyclase
c) Blocking DNA synthesis
d) Increasing ATP
Answer: b) Inhibiting adenylate cyclase
- Methadone causes hyperpolarization by:
a) Sodium influx
b) Potassium efflux
c) Calcium influx
d) Chloride influx
Answer: b) Potassium efflux
- Methadone decreases neurotransmitter release by reducing:
a) Sodium
b) Calcium
c) Potassium
d) Chloride
Answer: b) Calcium
- Methadone is commonly used in:
a) Asthma
b) Opioid dependence
c) Hypertension
d) Diabetes
Answer: b) Opioid dependence
- Methadone has which duration of action?
a) Short
b) Moderate
c) Long
d) Ultra-short
Answer: c) Long
- A unique adverse effect of methadone is:
a) Hypoglycemia
b) QT prolongation
c) Hypercalcemia
d) Renal failure
Answer: b) QT prolongation
- Methadone is metabolized mainly in the:
a) Kidney
b) Liver
c) Lung
d) Brain
Answer: b) Liver
- Compared to buprenorphine, methadone is:
a) Partial agonist
b) Full agonist
c) Antagonist
d) Inverse agonist
Answer: b) Full agonist
- Methadone reduces release of which neurotransmitter?
a) Glutamate
b) Insulin
c) Thyroxine
d) Cortisol
Answer: a) Glutamate
- Methadone is eliminated via:
a) Liver only
b) Kidney and feces
c) Lungs
d) Skin
Answer: b) Kidney and feces
FAQs
What is the mechanism of action of methadone?
It is a μ-opioid receptor agonist and NMDA receptor antagonist that reduces neuronal excitability and pain transmission.
Why is methadone used in opioid dependence?
It prevents withdrawal symptoms and reduces cravings due to its long duration.
What makes methadone different from other opioids?
Its NMDA receptor antagonism and long half-life.
What is a major cardiac risk of methadone?
QT prolongation leading to arrhythmias.
Why is methadone dosing carefully monitored?
Due to its long half-life and risk of accumulation.
Can methadone cause dependence?
Yes, it is an opioid and can lead to dependence.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics – Opioids
https://accessmedicine.mhmedical.com/book.aspx?bookid=3191
Katzung: Basic and Clinical Pharmacology – Opioid Analgesics
https://accessmedicine.mhmedical.com/content.aspx?bookid=3382
Tripathi: Essentials of Medical Pharmacology – Opioids
https://www.jaypeedigital.com
Harrison’s Principles of Internal Medicine – Substance Use Disorders
https://accessmedicine.mhmedical.com

