Table of Contents
Introduction
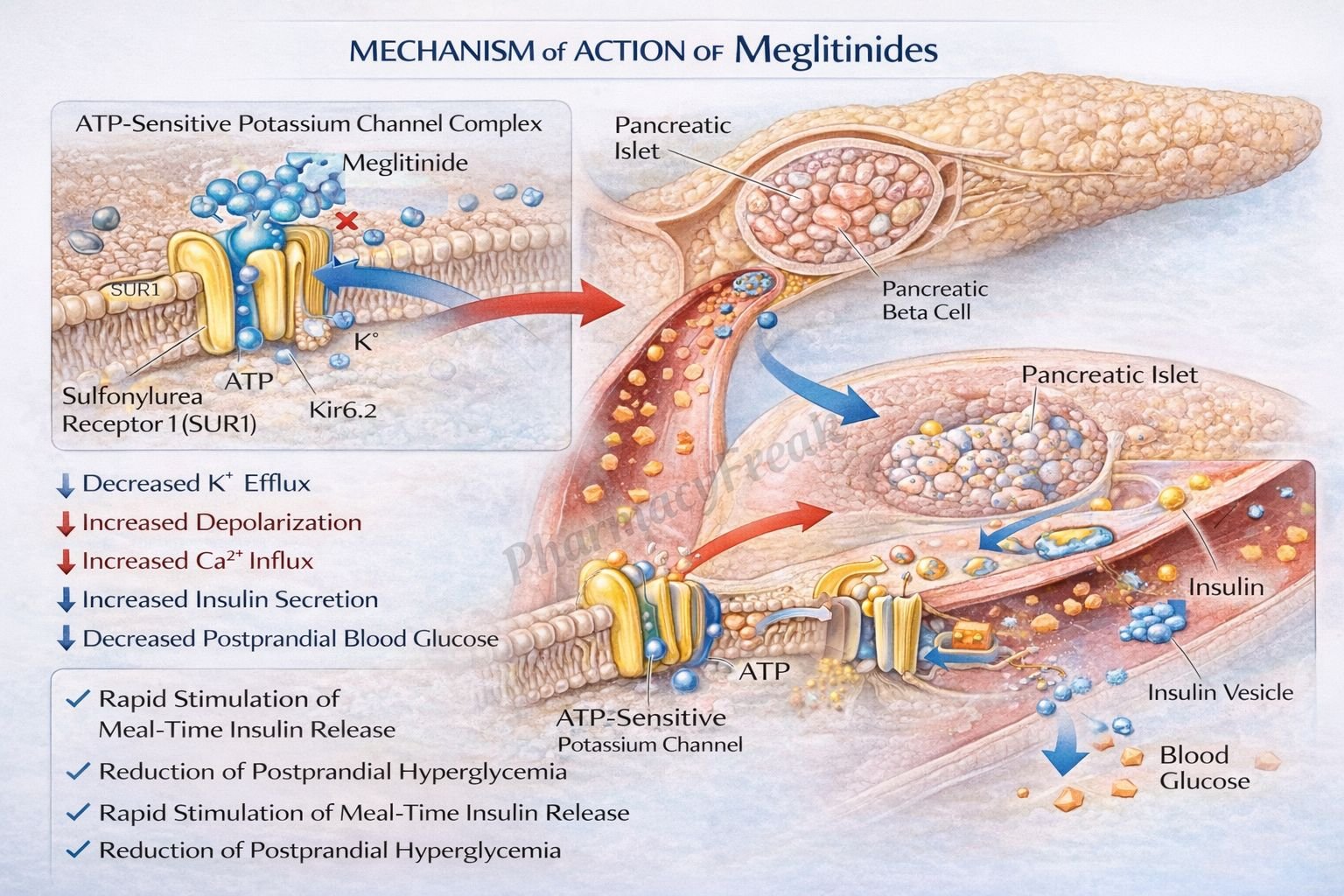
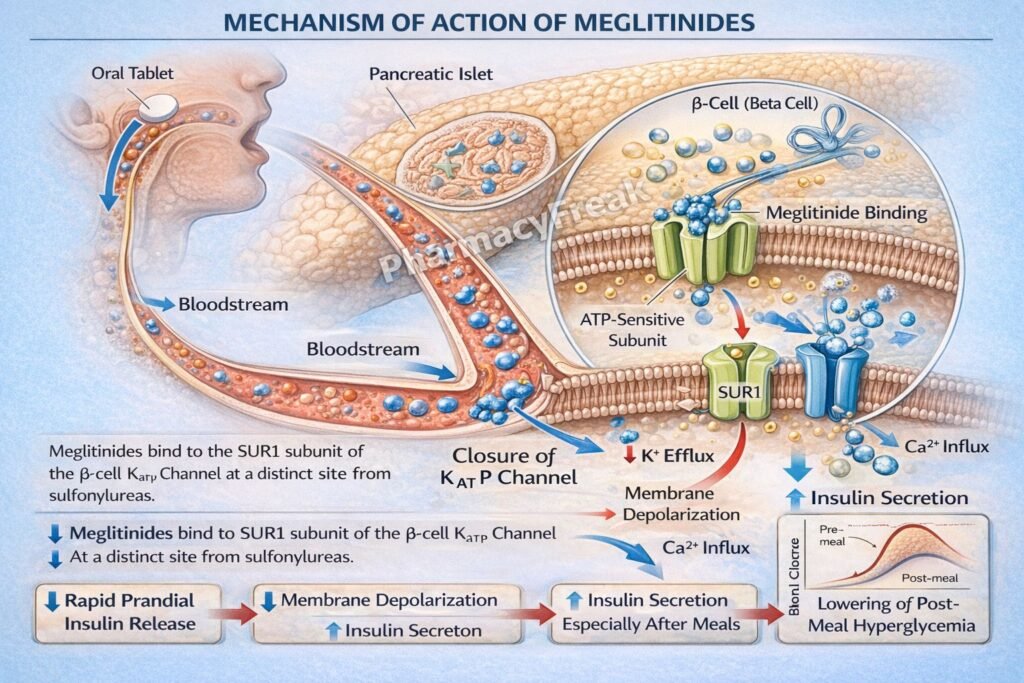
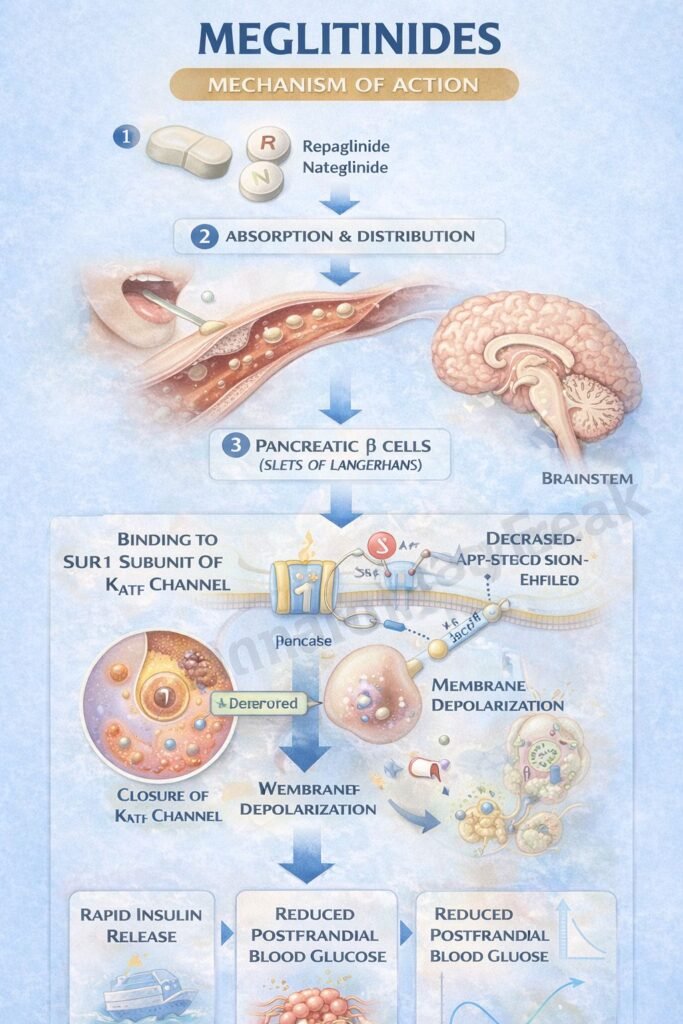
Meglitinides are a class of oral antidiabetic drugs used in the management of type 2 diabetes mellitus. Common agents include repaglinide and nateglinide. They are insulin secretagogues that stimulate rapid, short-acting insulin release from pancreatic β-cells. Meglitinides are particularly effective in controlling postprandial hyperglycemia due to their quick onset and short duration of action.
Mechanism of Action (Step-wise)
- Meglitinides bind to ATP-sensitive potassium (K⁺ATP) channels on pancreatic β-cell membranes.
- They bind at a site distinct from sulfonylureas but produce a similar effect.
- Binding causes closure of K⁺ATP channels.
- This leads to depolarization of the β-cell membrane.
- Depolarization opens voltage-gated calcium channels.
- Calcium influx into the β-cell increases intracellular calcium concentration.
- Elevated calcium triggers exocytosis of insulin-containing granules.
- This results in increased insulin secretion.
- The effect is glucose-dependent to some extent and primarily targets postprandial glucose spikes.
A key exam point is that meglitinides stimulate insulin release by closing K⁺ATP channels with rapid onset and short duration.
Pharmacokinetics
Meglitinides are administered orally and are rapidly absorbed from the gastrointestinal tract. They have a quick onset of action and a short half-life, which allows dosing before meals. They undergo extensive hepatic metabolism, primarily via cytochrome P450 enzymes, and are excreted mainly through bile. Because of their short duration, they have a lower risk of prolonged hypoglycemia compared to sulfonylureas.
Clinical Uses
Meglitinides are used in type 2 diabetes mellitus, particularly for patients with postprandial hyperglycemia. They are useful in patients with irregular meal schedules because they can be taken before meals and omitted if a meal is skipped. They are often used as monotherapy or in combination with other antidiabetic agents such as metformin.
Adverse Effects
The main adverse effect of meglitinides is hypoglycemia, although it is generally less severe than with sulfonylureas due to shorter duration of action. Weight gain may also occur due to increased insulin levels. Other side effects include mild gastrointestinal disturbances and rare hypersensitivity reactions. Caution is required in hepatic impairment due to liver metabolism.
Comparative Analysis
| Feature | Meglitinides | Sulfonylureas | Metformin |
|---|---|---|---|
| Mechanism | K⁺ATP channel closure | K⁺ATP channel closure | Decreases hepatic glucose production |
| Onset | Rapid | Slower | Moderate |
| Duration | Short | Long | Long |
| Hypoglycemia risk | Moderate (short-lived) | High | Low |
| Weight gain | Yes | Yes | No |
| Use | Postprandial control | Fasting + postprandial | First-line therapy |
Meglitinides differ from sulfonylureas mainly in their rapid onset and short duration, making them ideal for controlling postprandial glucose levels. Metformin, in contrast, does not stimulate insulin secretion but reduces hepatic glucose production and improves insulin sensitivity.
MCQs
- Meglitinides act by:
a) Increasing insulin sensitivity
b) Blocking glucose absorption
c) Stimulating insulin secretion
d) Inhibiting glucagon
Answer: c) Stimulating insulin secretion
- The primary site of action of meglitinides is:
a) Liver
b) Muscle
c) Pancreatic β-cells
d) Kidney
Answer: c) Pancreatic β-cells
- Meglitinides close which channels?
a) Sodium channels
b) Potassium ATP channels
c) Calcium channels
d) Chloride channels
Answer: b) Potassium ATP channels
- Closure of K⁺ATP channels leads to:
a) Hyperpolarization
b) Depolarization
c) No change
d) Repolarization
Answer: b) Depolarization
- Insulin release is triggered by:
a) Sodium influx
b) Calcium influx
c) Potassium influx
d) Chloride influx
Answer: b) Calcium influx
- Meglitinides are best for controlling:
a) Fasting glucose
b) Postprandial glucose
c) Basal insulin
d) Night glucose
Answer: b) Postprandial glucose
- Compared to sulfonylureas, meglitinides have:
a) Longer duration
b) Shorter duration
c) Same duration
d) No effect
Answer: b) Shorter duration
- A major adverse effect is:
a) Hypoglycemia
b) Hyperglycemia
c) Hypocalcemia
d) Hypernatremia
Answer: a) Hypoglycemia
- Meglitinides are metabolized mainly in the:
a) Kidney
b) Liver
c) Lung
d) Brain
Answer: b) Liver
- Meglitinides are taken:
a) Once daily
b) Before meals
c) After meals
d) At bedtime
Answer: b) Before meals
- Which drug class has a similar mechanism?
a) Biguanides
b) Sulfonylureas
c) Thiazolidinediones
d) DPP-4 inhibitors
Answer: b) Sulfonylureas
- Meglitinides are useful in patients with:
a) Type 1 diabetes
b) Irregular meals
c) Severe renal failure only
d) Hypoglycemia
Answer: b) Irregular meals
FAQs
What is the mechanism of action of meglitinides?
They stimulate insulin secretion by closing K⁺ATP channels in pancreatic β-cells.
How are meglitinides different from sulfonylureas?
They have a faster onset and shorter duration of action.
Why are meglitinides taken before meals?
To control postprandial glucose spikes.
What is the main adverse effect of meglitinides?
Hypoglycemia.
Can meglitinides cause weight gain?
Yes, due to increased insulin secretion.
Are meglitinides used in type 1 diabetes?
No, they require functioning β-cells.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics – Antidiabetic Drugs
https://accessmedicine.mhmedical.com/book.aspx?bookid=3191
Katzung: Basic and Clinical Pharmacology – Antidiabetic Agents
https://accessmedicine.mhmedical.com/content.aspx?bookid=3382
Tripathi: Essentials of Medical Pharmacology – Antidiabetic Drugs
https://www.jaypeedigital.com
Harrison’s Principles of Internal Medicine – Diabetes Mellitus
https://accessmedicine.mhmedical.com

