Introduction
Local anesthetics are drugs that reversibly block nerve conduction, producing loss of sensation in a specific area without affecting consciousness. They are widely used in minor surgical procedures, dental practice, regional anesthesia, and pain management. The fundamental mechanism involves inhibition of voltage-gated sodium channels in nerve fibers, preventing the initiation and propagation of action potentials.
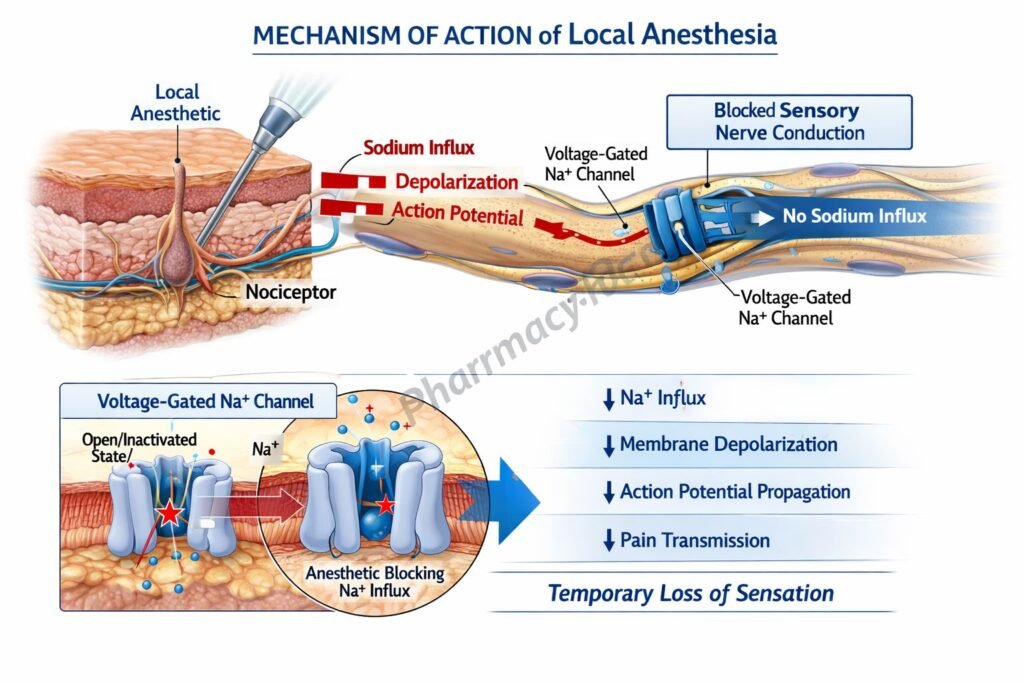
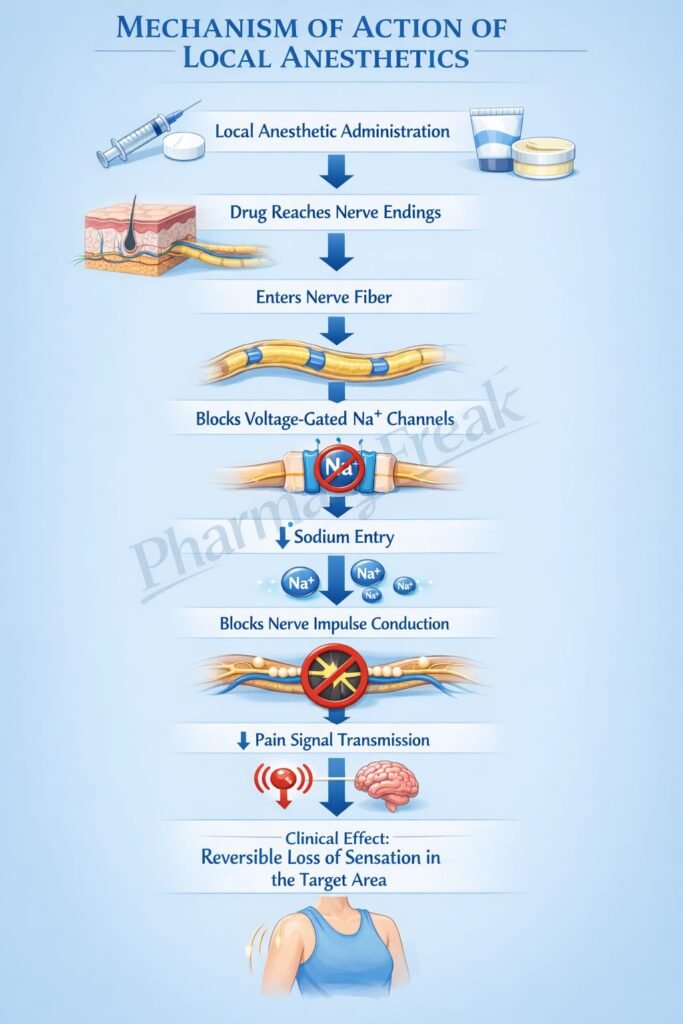
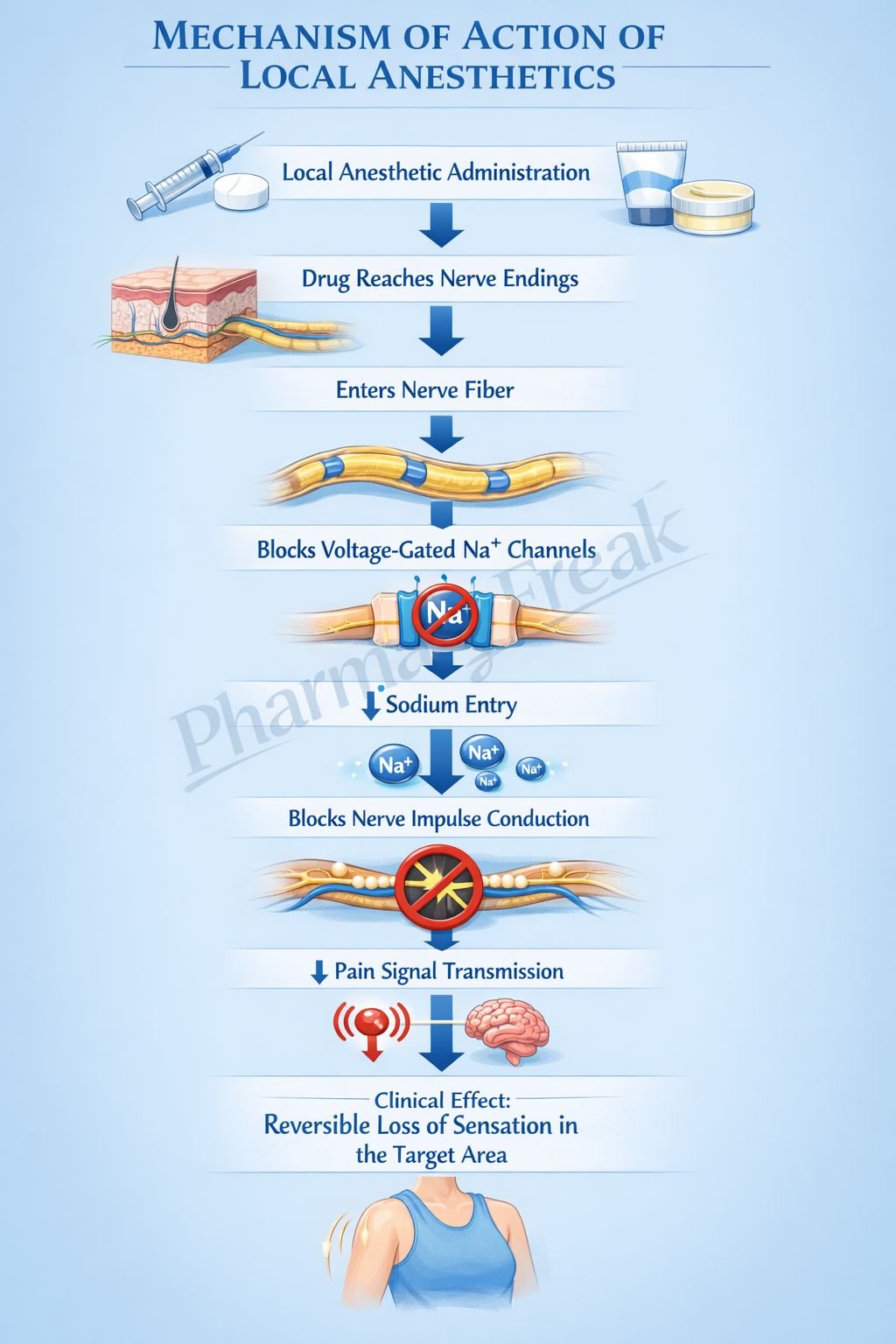
Mechanism of Action (Step-wise)
- Local anesthetics diffuse across the neuronal membrane in their uncharged (lipid-soluble) form.
- Inside the axoplasm, a portion of the drug becomes ionized.
- The ionized form binds to the intracellular portion of voltage-gated sodium channels (Nav channels).
- This binding stabilizes the inactivated state of sodium channels.
- As a result, sodium influx during depolarization is blocked.
- This prevents the generation of action potentials.
- Conduction of nerve impulses is therefore inhibited.
- Smaller, myelinated fibers (pain fibers A-delta and C fibers) are blocked first, followed by larger fibers.
- The effect is reversible once the drug diffuses away from the site of action.
A key exam concept is “use-dependent blockade,” meaning local anesthetics preferentially block rapidly firing nerves because sodium channels are more frequently in the open or inactivated state.
Pharmacokinetics
Local anesthetics are administered via topical, infiltration, nerve block, epidural, or spinal routes. They are classified into ester-type (e.g., procaine) and amide-type (e.g., lidocaine, bupivacaine). Ester anesthetics are rapidly hydrolyzed by plasma cholinesterases, whereas amide anesthetics are metabolized in the liver. Lipid solubility, protein binding, and pKa determine potency, duration, and onset. Drugs with higher lipid solubility and protein binding (e.g., bupivacaine) have longer duration. Addition of vasoconstrictors such as epinephrine prolongs action by reducing systemic absorption.
Clinical Uses
Local anesthetics are used in a wide range of procedures. These include topical anesthesia for mucous membranes, infiltration anesthesia for minor surgical procedures, peripheral nerve blocks for regional anesthesia, epidural and spinal anesthesia for surgeries and obstetrics, and management of acute and chronic pain. Lidocaine is also used intravenously as an antiarrhythmic agent.
Adverse Effects
Adverse effects are primarily related to systemic toxicity, especially when high doses or accidental intravascular injection occurs. Central nervous system toxicity may present as circumoral numbness, tinnitus, seizures, or CNS depression. Cardiovascular toxicity includes hypotension, arrhythmias, and cardiac depression, particularly with bupivacaine. Allergic reactions are more common with ester anesthetics due to para-aminobenzoic acid (PABA) formation. Methemoglobinemia can occur with certain agents such as prilocaine.
Comparative Analysis
| Feature | Ester Local Anesthetics | Amide Local Anesthetics |
|---|---|---|
| Examples | Procaine, Tetracaine | Lidocaine, Bupivacaine |
| Metabolism | Plasma cholinesterase | Hepatic metabolism |
| Duration | Shorter | Longer |
| Allergy risk | Higher (PABA formation) | Lower |
| Stability | Less stable | More stable |
Ester anesthetics are rapidly broken down in plasma, resulting in shorter duration and higher allergy risk. Amide anesthetics are more commonly used clinically because of their longer duration and lower incidence of hypersensitivity reactions.
MCQs
- Local anesthetics primarily act by blocking:
a) Calcium channels
b) Sodium channels
c) Potassium channels
d) Chloride channels
Answer: b) Sodium channels
- The site of action of local anesthetics is:
a) Extracellular receptor only
b) Intracellular portion of sodium channels
c) Mitochondria
d) Ribosomes
Answer: b) Intracellular portion of sodium channels
- Which fibers are blocked first by local anesthetics?
a) Large motor fibers
b) Sensory fibers
c) Pain fibers (A-delta and C)
d) Autonomic fibers only
Answer: c) Pain fibers (A-delta and C)
- Local anesthetics prevent nerve conduction by:
a) Increasing potassium efflux
b) Blocking sodium influx
c) Increasing calcium entry
d) Enhancing neurotransmitter release
Answer: b) Blocking sodium influx
- Use-dependent blockade means:
a) Drugs act only at rest
b) Drugs act only during sleep
c) More blockade in rapidly firing nerves
d) Only motor nerves are blocked
Answer: c) More blockade in rapidly firing nerves
- Which class is metabolized in the liver?
a) Ester anesthetics
b) Amide anesthetics
c) Both equally
d) None
Answer: b) Amide anesthetics
- Ester anesthetics are metabolized by:
a) Liver enzymes
b) Kidney
c) Plasma cholinesterases
d) Lungs
Answer: c) Plasma cholinesterases
- Addition of epinephrine to local anesthetics:
a) Shortens duration
b) Increases toxicity
c) Prolongs duration
d) Blocks metabolism
Answer: c) Prolongs duration
- Which adverse effect is associated with systemic toxicity?
a) Hyperglycemia
b) Seizures
c) Constipation
d) Rash only
Answer: b) Seizures
- Bupivacaine is most associated with:
a) Renal toxicity
b) Cardiotoxicity
c) Hepatotoxicity
d) Neurodegeneration
Answer: b) Cardiotoxicity
- Allergic reactions are more common with:
a) Amide anesthetics
b) Ester anesthetics
c) Both equally
d) None
Answer: b) Ester anesthetics
- Methemoglobinemia is associated with:
a) Lidocaine
b) Prilocaine
c) Bupivacaine
d) Procaine
Answer: b) Prilocaine
FAQs
What is the main mechanism of action of local anesthetics?
They block voltage-gated sodium channels, preventing action potential generation and nerve conduction.
Why do local anesthetics block pain before motor function?
Smaller, myelinated pain fibers are more sensitive than larger motor fibers.
What is use-dependent blockade?
Local anesthetics preferentially block frequently activated sodium channels.
Why is epinephrine added to local anesthetics?
It reduces systemic absorption and prolongs duration of action.
Which local anesthetics are safer in terms of allergy?
Amide anesthetics are safer because they do not form PABA.
What causes toxicity of local anesthetics?
High plasma levels due to overdose or accidental intravascular injection.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics – Local Anesthetics
https://accessmedicine.mhmedical.com/book.aspx?bookid=3191
Katzung: Basic and Clinical Pharmacology – Local Anesthetics
https://accessmedicine.mhmedical.com/content.aspx?bookid=3382
Tripathi: Essentials of Medical Pharmacology – Local Anesthetics
https://www.jaypeedigital.com
Harrison’s Principles of Internal Medicine – Pain Management
https://accessmedicine.mhmedical.com

