Table of Contents
Introduction
Imipramine is a tricyclic antidepressant (TCA) widely used in the management of major depressive disorder, anxiety disorders, and certain pediatric conditions such as nocturnal enuresis. It is one of the prototype TCAs and exhibits both antidepressant and sedative properties. Its pharmacological effects are primarily mediated through modulation of monoamine neurotransmitters in the central nervous system.
Mechanism of Action (Step-wise)
- Inhibition of Monoamine Reuptake
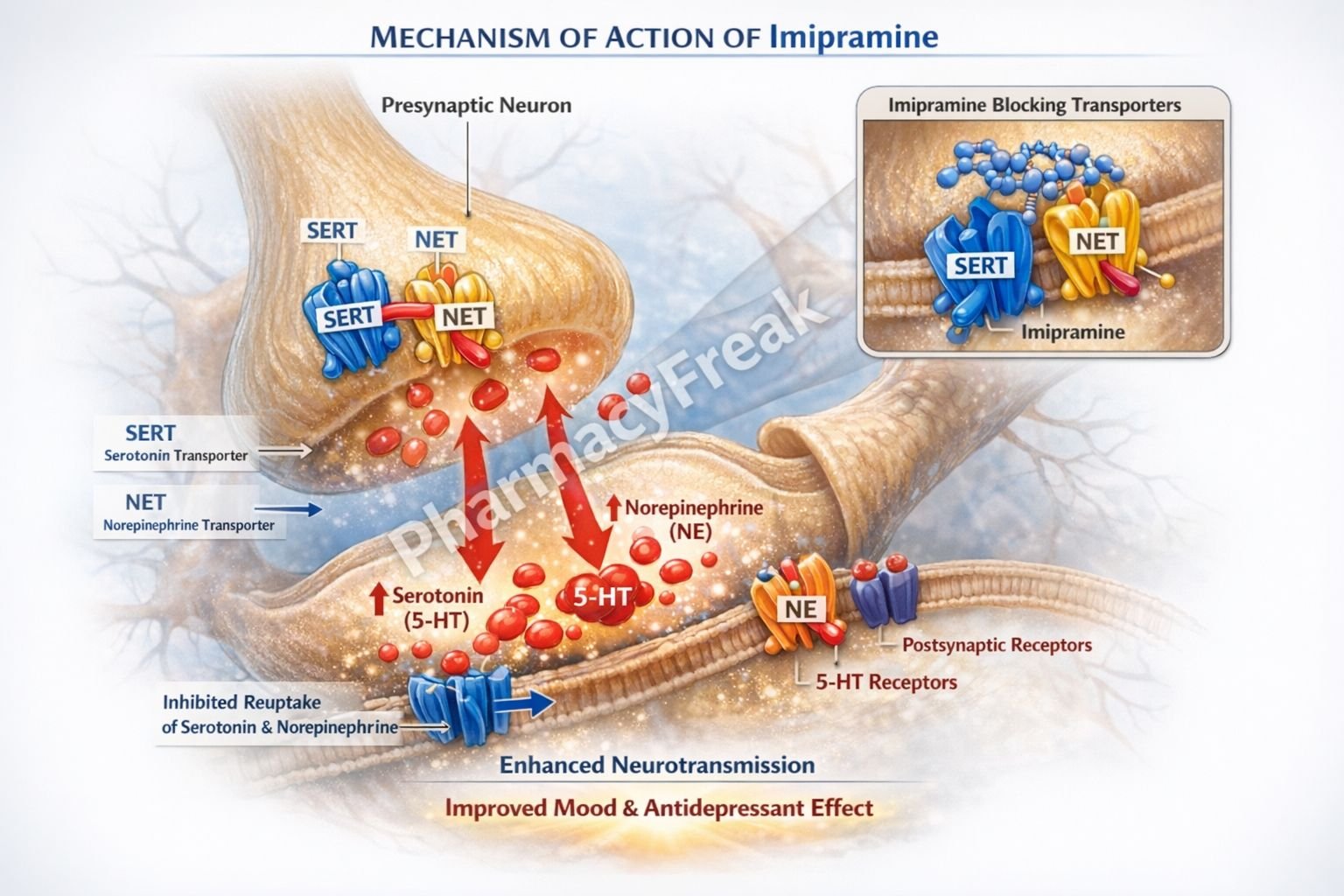
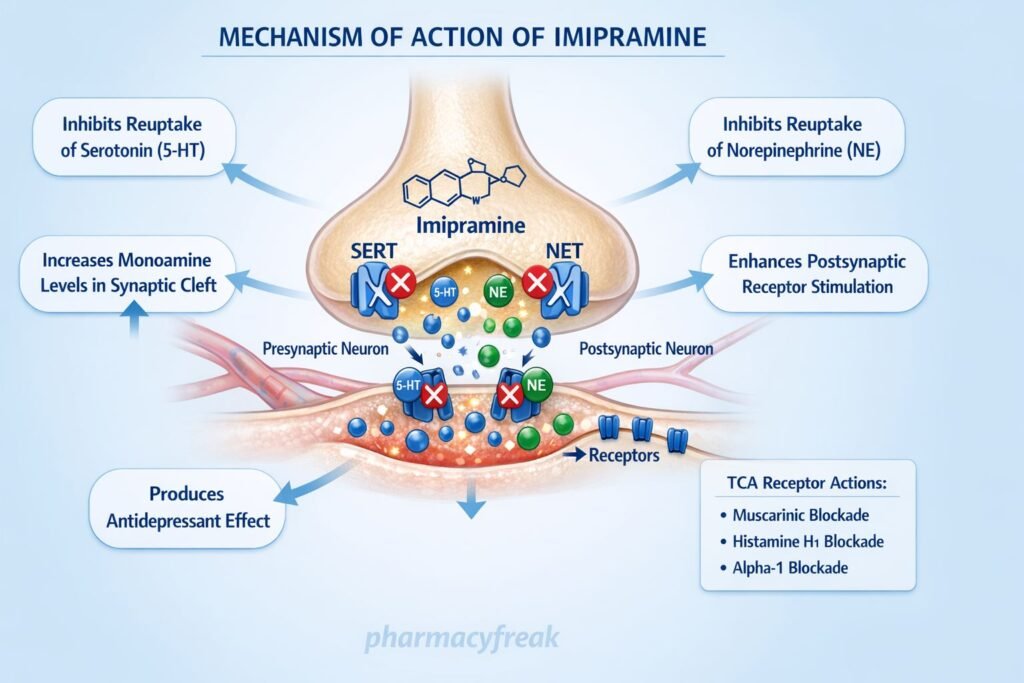
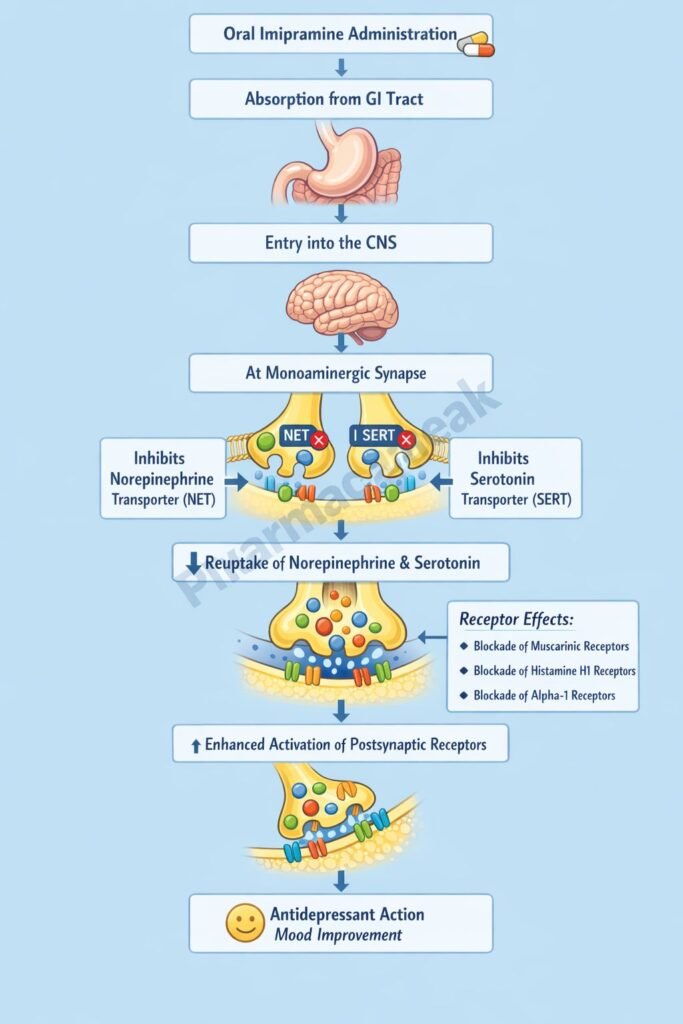
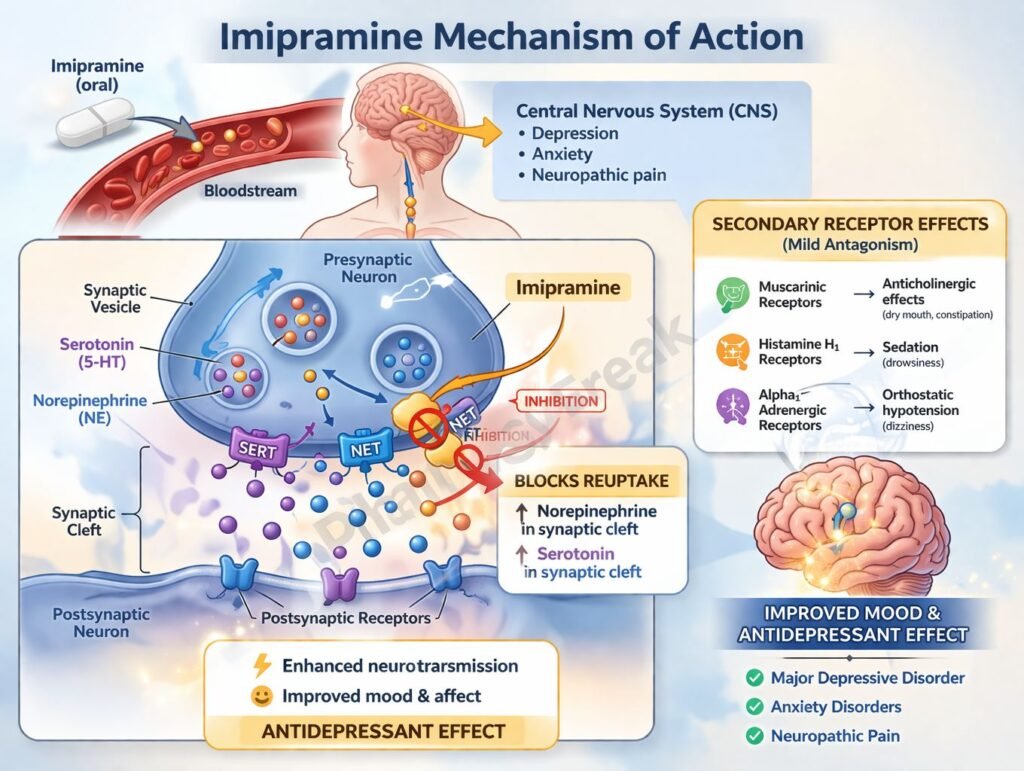
Imipramine inhibits the reuptake of norepinephrine (NE) and serotonin (5-HT) by blocking their respective transporters (NET and SERT) at presynaptic nerve terminals. - Increased Synaptic Neurotransmitter Levels
This inhibition leads to increased concentrations of NE and 5-HT in the synaptic cleft. - Enhanced Neurotransmission
Elevated monoamine levels enhance stimulation of postsynaptic receptors, contributing to antidepressant effects. - Downregulation of Receptors (Chronic Effect)
Long-term use leads to downregulation and desensitization of β-adrenergic and serotonin receptors, which is associated with therapeutic efficacy. - Anticholinergic Activity
Imipramine blocks muscarinic receptors, contributing to side effects such as dry mouth and urinary retention. - Antihistaminic Effect
It blocks H1 receptors, leading to sedation. - Alpha-1 Adrenergic Blockade
Causes vasodilation and may lead to orthostatic hypotension.
Pharmacokinetics
- Absorption: Well absorbed after oral administration
- First-pass metabolism: Significant hepatic metabolism
- Active metabolite: Desipramine (more selective for norepinephrine reuptake inhibition)
- Protein Binding: High
- Half-life: 8–20 hours (longer for metabolite)
- Excretion: Renal (as metabolites)
Clinical Uses
- Major depressive disorder
- Anxiety disorders
- Panic disorder
- Nocturnal enuresis (bedwetting) in children
- Neuropathic pain (off-label)
Adverse Effects
- Anticholinergic effects: dry mouth, blurred vision, constipation, urinary retention
- Sedation (due to H1 blockade)
- Orthostatic hypotension (α1 blockade)
- Cardiotoxicity (arrhythmias, conduction defects)
- Weight gain
- CNS effects: confusion, delirium (especially in elderly)
Comparative Analysis
| Feature | Imipramine | Amitriptyline | Fluoxetine |
|---|---|---|---|
| Class | TCA | TCA | SSRI |
| Mechanism | Blocks NE & 5-HT reuptake | Blocks NE & 5-HT reuptake | Selective 5-HT reuptake inhibition |
| Sedation | Moderate | High | Low |
| Anticholinergic effects | Moderate | High | Minimal |
| Cardiotoxicity | Present | High | Low |
| Use in enuresis | Yes | No | No |
Imipramine is less sedating and has slightly fewer anticholinergic effects compared to amitriptyline but still carries significant TCA-related risks. Compared to SSRIs like fluoxetine, it has broader receptor activity but a less favorable safety profile.
MCQs
- Imipramine primarily inhibits:
a) Dopamine reuptake
b) GABA receptors
c) Norepinephrine and serotonin reuptake
d) NMDA receptors
Answer: c) Norepinephrine and serotonin reuptake - Active metabolite of imipramine:
a) Nortriptyline
b) Desipramine
c) Fluoxetine
d) Sertraline
Answer: b) Desipramine - Which receptor blockade causes dry mouth?
a) Dopamine
b) Muscarinic
c) NMDA
d) GABA
Answer: b) Muscarinic - Sedation with imipramine is due to:
a) H2 blockade
b) H1 blockade
c) Beta blockade
d) Dopamine blockade
Answer: b) H1 blockade - Orthostatic hypotension is due to:
a) Alpha-1 blockade
b) Beta-2 blockade
c) Serotonin blockade
d) Calcium channel blockade
Answer: a) Alpha-1 blockade - Imipramine is used in:
a) Hypertension
b) Depression
c) Diabetes
d) Asthma
Answer: b) Depression - Cardiotoxicity is a concern because:
a) Sodium channel blockade
b) Calcium channel activation
c) Potassium depletion
d) Insulin release
Answer: a) Sodium channel blockade - Which class does imipramine belong to?
a) SSRI
b) MAOI
c) TCA
d) Benzodiazepine
Answer: c) TCA - Imipramine increases which neurotransmitters?
a) Dopamine only
b) GABA
c) NE and 5-HT
d) Acetylcholine
Answer: c) NE and 5-HT - Major side effect in elderly:
a) Hypertension
b) Delirium
c) Hyperglycemia
d) Hair loss
Answer: b) Delirium
FAQs
- What is the primary mechanism of action of imipramine?
It inhibits reuptake of norepinephrine and serotonin, increasing their synaptic levels. - Why does imipramine cause sedation?
Due to histamine H1 receptor blockade. - What is the role of desipramine?
It is an active metabolite with stronger norepinephrine reuptake inhibition. - Why is imipramine used in enuresis?
It reduces bladder contractility and increases sphincter tone. - What makes TCAs risky in overdose?
They cause cardiac arrhythmias due to sodium channel blockade. - Is imipramine safer than SSRIs?
No, SSRIs generally have a better safety profile.


