Table of Contents
Introduction
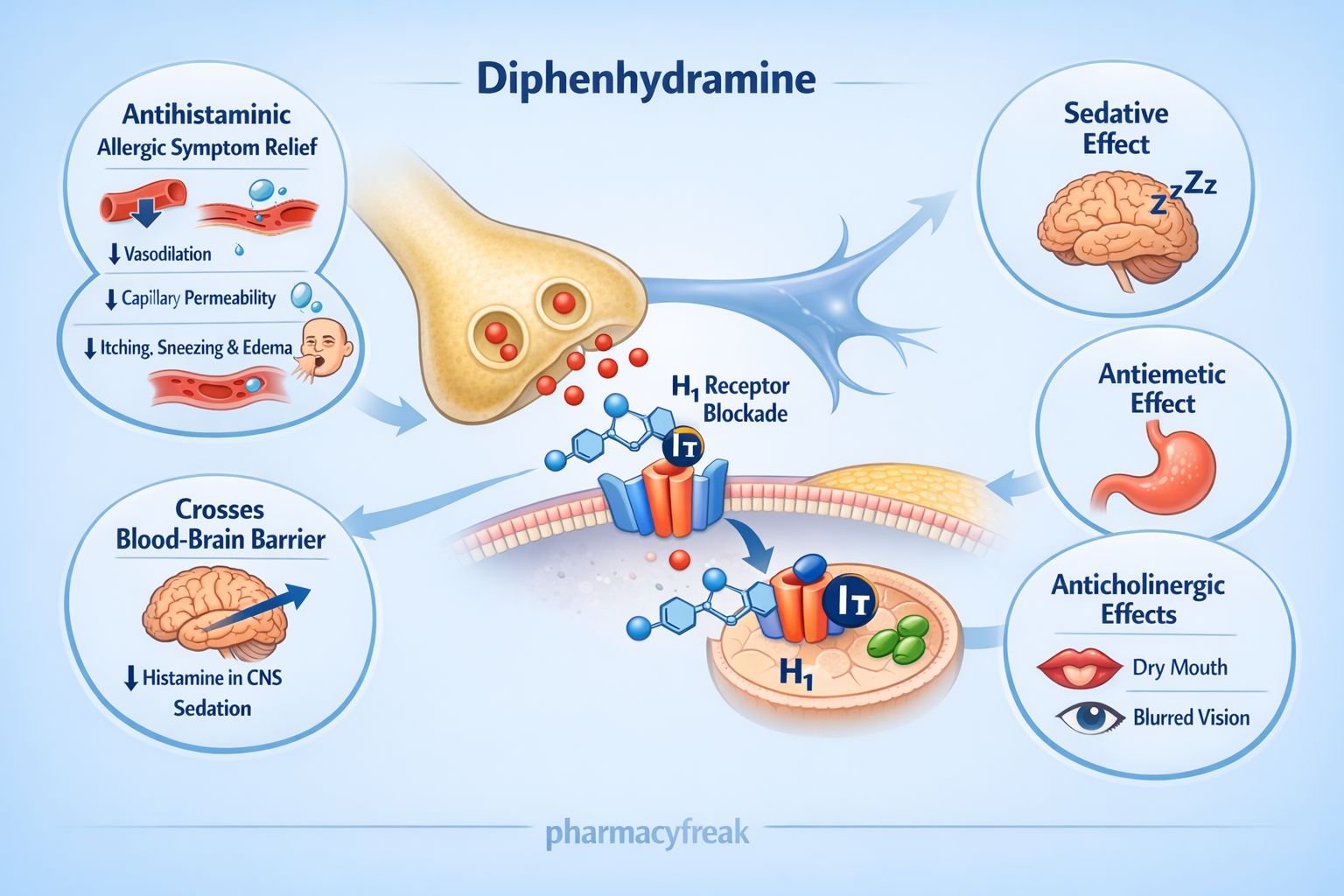
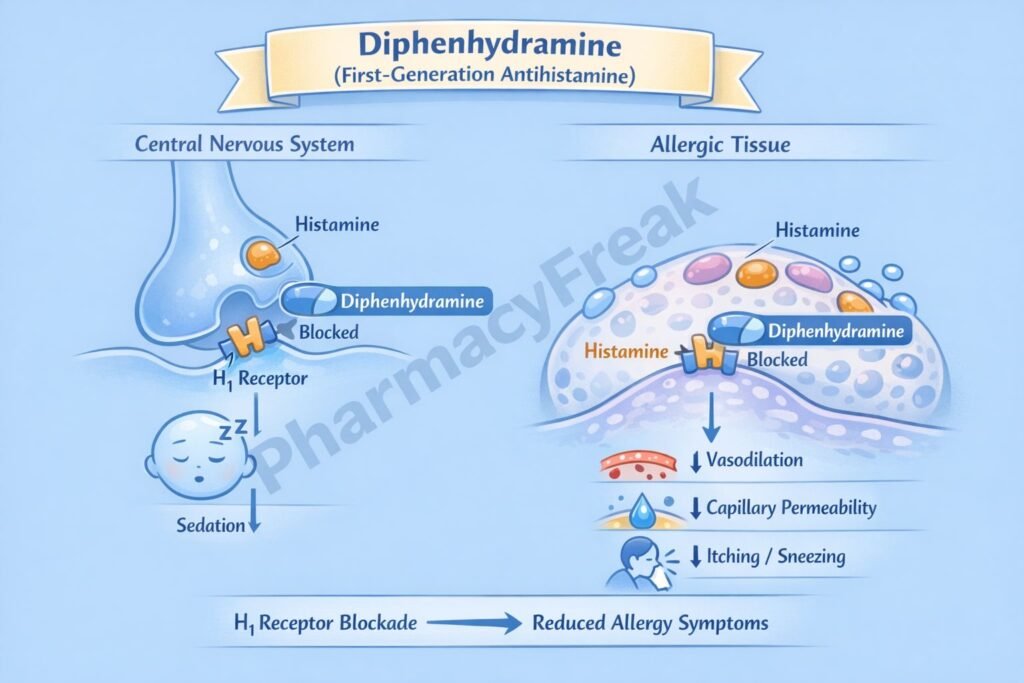
Diphenhydramine is a first-generation H₁ antihistamine belonging to the ethanolamine class. It is widely used for the treatment of allergic conditions and is also commonly employed as a sedative, antiemetic, antitussive, and antiparkinsonian adjunct. Because of its strong central anticholinergic and sedative properties, diphenhydramine is a high-yield drug in pharmacology, medicine, nursing, and emergency medicine examinations.
Mechanism of Action (Step-wise)
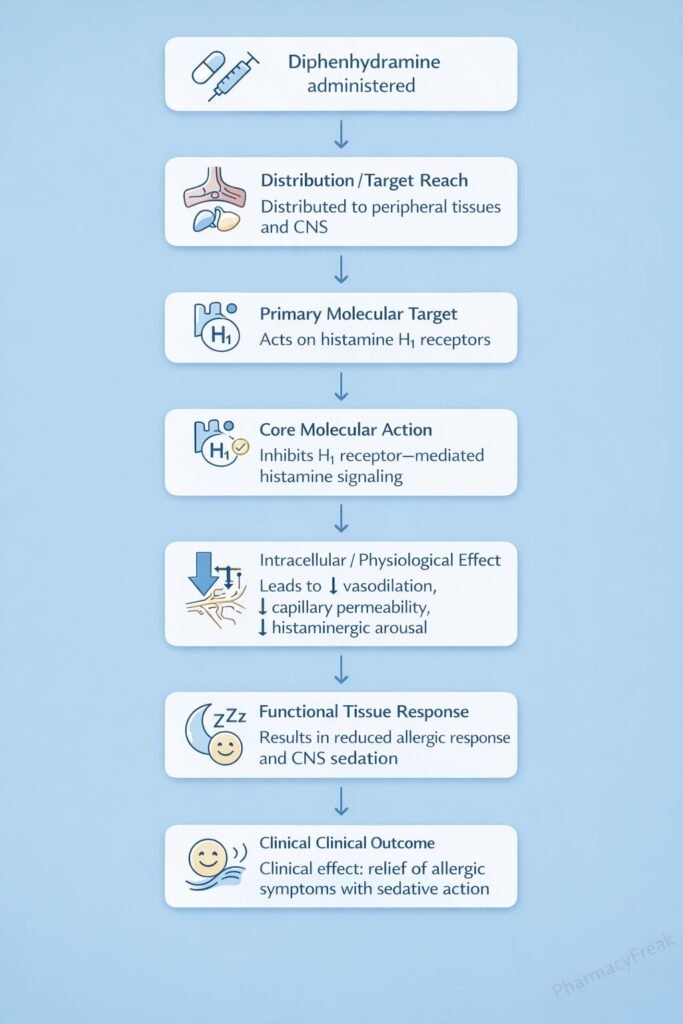
Diphenhydramine produces its pharmacological effects primarily through histamine and muscarinic receptor blockade.
Step-wise mechanism:
- Histamine Release in Allergic Reactions
In allergic states, mast cells release histamine, which acts on H₁ receptors to cause vasodilation, increased capillary permeability, itching, and bronchoconstriction. - H₁ Receptor Antagonism
Diphenhydramine competitively blocks histamine H₁ receptors in peripheral tissues. - Reduction of Allergic Symptoms
H₁ blockade reduces:- Vasodilation
- Capillary permeability
- Edema
- Pruritus
- Central Nervous System Penetration
Due to high lipophilicity, diphenhydramine readily crosses the blood–brain barrier. - Sedative Effect
Central H₁ receptor blockade in the brain produces sedation and drowsiness. - Anticholinergic (Antimuscarinic) Action
Diphenhydramine blocks muscarinic receptors, contributing to:- Anti–motion sickness effects
- Antiparkinsonian effects
- Antiemetic action
- Suppression of Vestibular Stimulation
Combined H₁ and muscarinic blockade suppresses vestibular signaling to the vomiting center.
Pharmacokinetics
- Absorption: Well absorbed orally
- Distribution: Widely distributed; crosses blood–brain barrier
- Metabolism: Hepatic metabolism (CYP450 enzymes)
- Elimination: Renal excretion of metabolites
- Half-life: Approximately 4–8 hours
- Onset of action: 15–60 minutes
Clinical Uses
Diphenhydramine is used in a wide range of allergic and non-allergic conditions:
- Allergic rhinitis (hay fever)
- Urticaria and pruritus
- Motion sickness
- Vertigo and vestibular disorders
- Insomnia (short-term)
- Acute dystonic reactions (drug-induced EPS)
- Parkinson disease (adjunct)
- Antitussive in cough syrups
Adverse Effects
Adverse effects are mainly due to CNS penetration and anticholinergic activity:
- Central nervous system:
- Sedation
- Drowsiness
- Dizziness
- Confusion (elderly)
- Anticholinergic effects:
- Dry mouth
- Blurred vision
- Constipation
- Urinary retention
- Tachycardia
- Paradoxical excitation (children, rare)
Diphenhydramine should be used cautiously in elderly patients and those with glaucoma or prostatic hypertrophy.
Comparative Analysis (must include a table + explanation)
Comparison of Antihistamines
| Feature | Diphenhydramine | Loratadine | Cetirizine |
|---|---|---|---|
| Generation | First | Second | Second |
| CNS penetration | High | Minimal | Low |
| Sedation | High | None | Mild |
| Anticholinergic effects | Prominent | None | Minimal |
| Motion sickness use | Yes | No | No |
Explanation:
Diphenhydramine differs from second-generation antihistamines by its strong central and anticholinergic effects. While this limits its daytime use due to sedation, it provides advantages in motion sickness, acute dystonia, and short-term insomnia.
MCQs (10–15)
- Diphenhydramine primarily blocks which receptor?
a) H₂ receptor
b) H₁ receptor
c) Dopamine receptor
d) Serotonin receptor
Answer: b) H₁ receptor
- Diphenhydramine belongs to which generation of antihistamines?
a) Third
b) Second
c) First
d) Atypical
Answer: c) First
- Sedation caused by diphenhydramine is due to:
a) Dopamine blockade
b) Peripheral H₁ blockade
c) Central H₁ blockade
d) Serotonin inhibition
Answer: c) Central H₁ blockade
- Diphenhydramine is useful in motion sickness because of its:
a) Opioid action
b) Anticholinergic effect
c) Dopamine antagonism
d) GABA agonism
Answer: b) Anticholinergic effect
- Which adverse effect is most characteristic of diphenhydramine?
a) QT prolongation
b) Sedation
c) Nephrotoxicity
d) Hepatotoxicity
Answer: b) Sedation
- Diphenhydramine can be used to treat:
a) Tardive dyskinesia
b) Acute dystonia
c) Schizophrenia
d) Epilepsy
Answer: b) Acute dystonia
- Diphenhydramine crosses the blood–brain barrier because it is:
a) Water soluble
b) Ionized
c) Lipophilic
d) Protein bound
Answer: c) Lipophilic
- Diphenhydramine should be avoided in patients with:
a) Allergic rhinitis
b) Motion sickness
c) Glaucoma
d) Urticaria
Answer: c) Glaucoma
- Which property distinguishes diphenhydramine from loratadine?
a) H₁ blockade
b) Sedation
c) Antiallergic effect
d) Oral absorption
Answer: b) Sedation
- Diphenhydramine also acts as a:
a) Beta blocker
b) Anticholinergic
c) Alpha agonist
d) COX inhibitor
Answer: b) Anticholinergic
FAQs (minimum 5)
- What is the primary mechanism of diphenhydramine?
Competitive antagonism of histamine H₁ receptors. - Why does diphenhydramine cause sedation?
Due to central H₁ receptor blockade in the brain. - Does diphenhydramine have anticholinergic effects?
Yes, contributing to its antiemetic and antiparkinsonian actions. - Is diphenhydramine safe in elderly patients?
Use cautiously due to risk of confusion and urinary retention. - Can diphenhydramine be used for sleep?
Yes, short-term use due to sedative effects. - Is diphenhydramine useful for asthma?
No, it does not relieve bronchoconstriction effectively.
References
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics
https://accessmedicine.mhmedical.com - Katzung BG. Basic and Clinical Pharmacology
https://accessmedicine.mhmedical.com - Tripathi KD. Essentials of Medical Pharmacology
https://www.jaypeebrothers.com - Harrison’s Principles of Internal Medicine
https://accessmedicine.mhmedical.com

