Table of Contents
Introduction
Colace is the brand name for docusate sodium, a stool softener widely used for the prevention and treatment of constipation. It is classified as a surfactant laxative and is commonly prescribed in patients who should avoid straining during defecation, such as post-surgical patients, individuals with hemorrhoids, cardiovascular disease, or postpartum patients. Colace is frequently tested in pharmacology and nursing examinations because of its unique mechanism as a stool softener rather than a stimulant laxative.

Mechanism of Action (Step-wise)
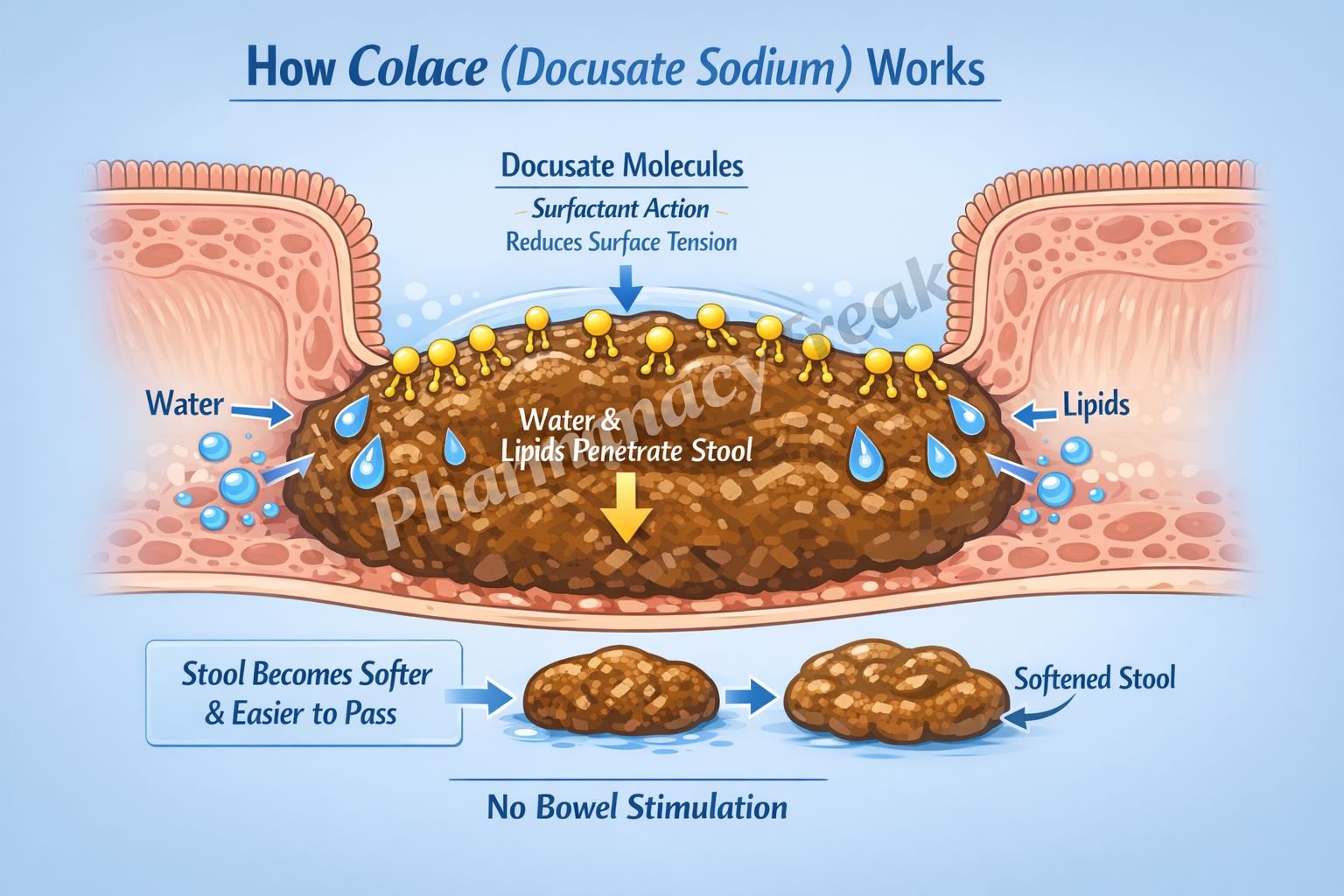
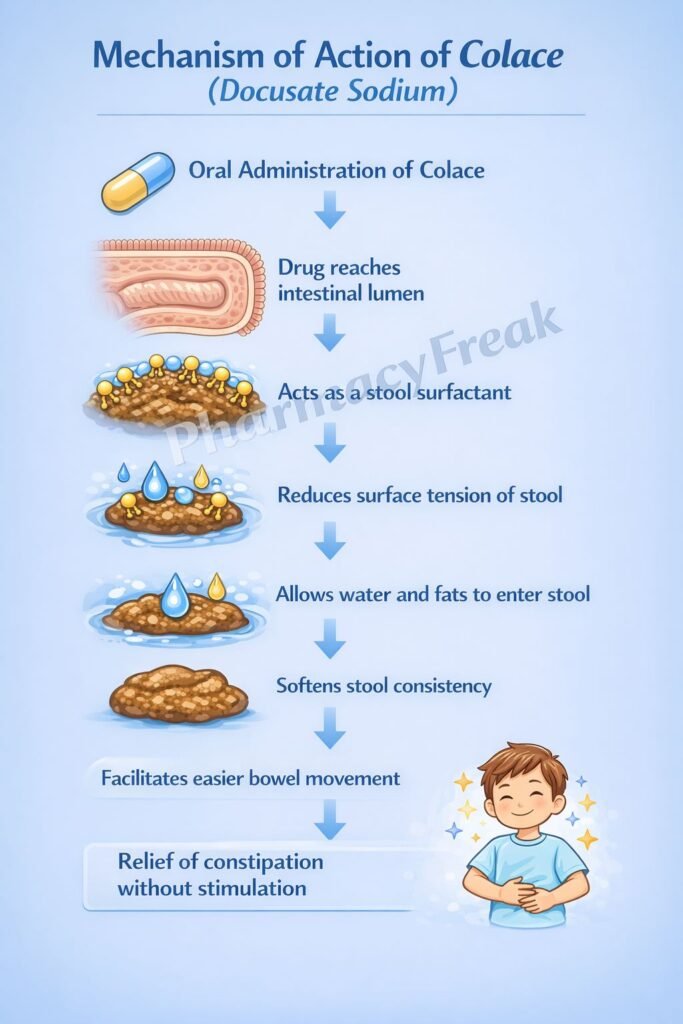
Colace (docusate sodium) facilitates bowel movements by softening stool through surfactant action.
Step-wise mechanism:
- Oral Administration and GI Transit
After oral or rectal administration, docusate reaches the intestinal lumen without significant systemic absorption. - Surfactant (Detergent) Action
Docusate acts as an anionic surfactant that lowers the surface tension of stool. - Increased Water Penetration
Reduced surface tension allows water and lipids to penetrate and mix with fecal matter. - Softening of Stool Consistency
Increased water content softens the stool and increases fecal bulk. - Facilitated Defecation
Softer stool passes more easily through the colon, reducing the need for straining. - No Direct Effect on Intestinal Motility
Colace does not stimulate peristalsis or intestinal smooth muscle contraction.
Pharmacokinetics
- Absorption: Minimal systemic absorption
- Distribution: Acts locally within the gastrointestinal tract
- Metabolism: Limited intestinal metabolism
- Elimination: Excreted in feces
- Onset of action: 12–72 hours
- Duration: Depends on stool hydration and continued use
Because of negligible systemic absorption, systemic adverse effects are rare.
Clinical Uses
Colace is primarily used for stool softening in conditions where straining should be avoided:
- Functional constipation
- Postoperative patients
- Hemorrhoids and anal fissures
- Post-myocardial infarction patients
- Pregnancy and postpartum constipation
- Opioid-induced constipation (adjunct therapy)
It is commonly used for prevention rather than treatment of severe constipation.
Adverse Effects
Colace is generally well tolerated. Adverse effects are uncommon and usually mild:
- Abdominal cramping
- Diarrhea (with excessive use)
- Throat irritation (liquid formulations)
- Nausea
Important note:
Chronic overuse may lead to electrolyte imbalance, although this is rare compared to stimulant laxatives.
Comparative Analysis (must include a table + explanation)
Comparison of Laxative Classes
| Feature | Colace (Docusate) | Stimulant Laxatives | Osmotic Laxatives |
|---|---|---|---|
| Primary action | Stool softening | Increases motility | Draws water into bowel |
| Onset | Slow (12–72 h) | Fast | Moderate |
| Effect on peristalsis | None | Strong | Mild |
| Risk of cramping | Low | High | Moderate |
| Use in prevention | Excellent | Poor | Moderate |
Explanation:
Colace differs from stimulant and osmotic laxatives by acting solely as a stool softener. It is ideal for long-term prevention of constipation and situations where intestinal stimulation is undesirable, but it is less effective for acute or severe constipation.
MCQs (10–15)
- Colace primarily acts by:
a) Stimulating intestinal motility
b) Inhibiting water absorption
c) Softening stool
d) Increasing bile secretion
Answer: c) Softening stool
- Colace is classified as a:
a) Stimulant laxative
b) Osmotic laxative
c) Bulk-forming laxative
d) Stool softener
Answer: d) Stool softener
- The mechanism of action of docusate involves:
a) Prostaglandin release
b) Surfactant activity
c) Chloride channel activation
d) Sodium-glucose transport inhibition
Answer: b) Surfactant activity
- Colace reduces constipation by increasing:
a) Intestinal motility
b) Electrolyte secretion
c) Water penetration into stool
d) Bile acid secretion
Answer: c) Water penetration into stool
- Which laxative does NOT stimulate peristalsis?
a) Senna
b) Bisacodyl
c) Lactulose
d) Colace
Answer: d) Colace
- The onset of action of Colace is typically:
a) 1–2 hours
b) 6 hours
c) 12–72 hours
d) Immediate
Answer: c) 12–72 hours
- Colace is most appropriate for:
a) Acute bowel obstruction
b) Severe fecal impaction
c) Prevention of constipation
d) Rapid bowel evacuation
Answer: c) Prevention of constipation
- Which patient should preferentially receive Colace?
a) Patient with acute abdomen
b) Post-MI patient
c) Patient with intestinal obstruction
d) Patient with infectious diarrhea
Answer: b) Post-MI patient
- Colace primarily acts in the:
a) Stomach
b) Small intestine
c) Colon
d) Rectum
Answer: c) Colon
- Chronic overuse of Colace may rarely cause:
a) Nephrotoxicity
b) Hepatotoxicity
c) Electrolyte imbalance
d) Bone loss
Answer: c) Electrolyte imbalance
FAQs (minimum 5)
- Is Colace a stimulant laxative?
No, it is a stool softener and does not stimulate bowel motility. - How long does Colace take to work?
Usually 12–72 hours after administration. - Can Colace be used daily?
Yes, it is safe for short-term daily use under medical supervision. - Is Colace effective for severe constipation?
No, it is more effective for prevention than for severe constipation. - Does Colace cause dependence?
No, it has a much lower risk of dependence compared to stimulant laxatives. - Can Colace be used in pregnancy?
Yes, it is commonly used when stool softening is required.
References
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics
https://accessmedicine.mhmedical.com - Katzung BG. Basic and Clinical Pharmacology
https://accessmedicine.mhmedical.com - Tripathi KD. Essentials of Medical Pharmacology
https://www.jaypeebrothers.com - Harrison’s Principles of Internal Medicine
https://accessmedicine.mhmedical.com

